Download
1 / 37
390 likes | 878 Vues
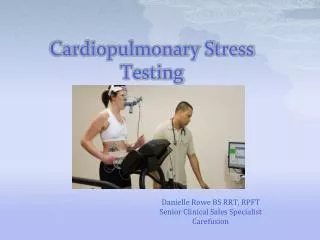
Cardiopulmonary Exercise Testing: Clinical Examples Darcy D. Marciniuk MD, FRCP(C), FCCP Division of Respirology, Critical Care and Sleep Medicine. Conflict of Interest Disclosure. Consultancy Fees / Advisory Boards

E N D
Cardiopulmonary Exercise Testing: Clinical Examples Darcy D. Marciniuk MD, FRCP(C), FCCP Division of Respirology, Critical Care and Sleep Medicine
Conflict of Interest Disclosure Consultancy Fees / Advisory Boards AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Health Canada, Health Quality Council, Novartis, Nycomed, Pfizer, Public Health Agency of Canada, Saskatchewan Medical Association, Saskatoon Health Region Research Funding AstraZeneca, Boehringer Ingelheim, Canadian Agency for Drugs and Technology in Health, Canadian Institute of Health Research, GlaxoSmithKline, Lung Association of Saskatchewan, Novartis, Nycomed, Pfizer, Saskatchewan Health Research Foundation, Saskatchewan Ministry of Health, Schering-Plough Speaker’s Bureau AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Pfizer Fiduciary Positions Canadian COPD Alliance, American College of Chest Physicians, Chest Foundation, Saskatchewan Lung Association Employee University of Saskatchewan
(↓= decreased; ↔ = unchanged from normal; ↑ = increased; v = variable)
Cardiopulmonary Exercise Testing Principles of Interpretation Address fundamental questions when interpreting exercise test results: • are the results normal or abnormal? • how limited is the patient? • what factors are responsible for the limitation? • what abnormal patterns of response are demonstrated? • what clinical disorders may result in these patterns of response?
Clinical Background – Case #1 64-yr-old male with COPD. Medication increased recently, but shortness of breath with exertion unchanged. No chest pain, no other significant history. Meds: tiotropium, salmeterol, salbutamol prn O/E: SaO2 96%, decreased breath sounds, all else normal ECG: no significant abnormalities CXR: hyperinflation, vascular deficiency Echocardiogram: normal ventricular function “Moderate COPD with significant limitation. Rehab referral” Cardiopulmonary Exercise Testing
Pulmonary Function BeforeAfter FVC (L) 3.38 3.59 (71% pred) (76% pred) FEV1 (L) 1.49 1.76 (50% pred) (59% pred) FEV1/FVC 44% 49% TLC (L) 6.86 (105% pred) RV (L) 3.36 (135% pred) Dlco (ml/min/mmHg)22.5 ( 65% pred) Cardiopulmonary Exercise Testing maximal incremental, room air, 10 watts/min cycle ergometer
Exercise Measurements RestEnd-Exercise%Pred Wmax(watts) -- 82 45 VO2(L/min)0.36 1.52 58 VO2 AT (L/min) -- 1.10 (>1.03) VE(L/min) 12.1 44.8 69 BR (L) -- 18.9 SaO2 (%) 97 98 HR (/min) 68 109 60 Dyspnea/Legs 0.5/0 5/5 ECG no arrhythmias or ischemic changes Cardiopulmonary Exercise Testing “I couldn’t do anymore - my breathing and legs”
Ventilatory Responses MVC (Normal) MVC (Lung Disease) Cardiopulmonary Exercise Testing
Flow (l/sec) Volume (l)
Interpretation physiologically sub-maximal study significant exercise limitation with reduced work and aerobic capacity although abnormal responses evident, respiratory system was not limiting mechanical ventilatory reserve, no oxygen desaturation, flow-volume curves no ECG/rhythm disturbances [prior normal echocardiogram] suggest heart rate and O2 pulse observations are consistent with a component of deconditioning Moderate COPD
Clinical Background – Case #2 16-yr-old female who presents with shortness of breath in gym class. Mother is concerned she is also not able to keep up with her peers (Mom was a university track & field competitor) No meds, no significant past/family history O/E: normal, no murmurs ECG: normal; CXR: normal PFT: normal MCT: PC20 > 32 mg/ml “Unexplained shortness of breath” Cardiopulmonary Exercise Testing
Exercise Measurements RestEnd-Exercise%Pred Wmax(watts) -- 65 47 VO2(L/min) 0.20 1.32 74 VE(L/min) 9.6 35.5 34 BR (L) -- 68.5 SaO2 (%) 99 96 HR (/min) 86 151 75 Dyspnea 2 9 Legs 0 3 Cardiopulmonary Exercise Testing “I Can’t Breath Anymore”
Interpretation physiologically sub-maximal study exercise limitation with reduced work (significant) and aerobic capacity (mild) respiratory system was not exercise limiting mechanical ventilatory reserve, no oxygen desaturation, respiratory responses not typical of a known disease process all other responses are normal other [… psychologic] contributors to the patient’s symptoms? Unexplained Dyspnea
Cardiopulmonary Exercise Testing Clinical Background – Case #3 • 56-yr-old male with Rheumatoid Arthritis x 5 years. 6 month history of decreasing exercise tolerance and increasing dry cough. • O/E: clubbed, reduced chest expansion, late inspiratory crackles, stigmata of RA • ECG: sinus tachycardia with RA enlargement • “56-year-old man with Rheumatoid Arthritis and Interstitial Lung Disease. ?transplant”
Cardiopulmonary Exercise Testing Pulmonary Function FVC (L) 1.82 53% pred FEV1 (L) 2.19 45% pred FEV1/FVC 83% TLC (L) 3.47 50% pred RV (L) 1.28 54% pred Dlco (ml/min/mmHg) 9.8 27% pred
Cardiopulmonary Exercise Testing Exercise Measurements RestEnd-Exercise%Pred Wmax(watts) -- 50 29 VO2(L/min) 0.34 1.07 44 VE(L/min) 20.1 68.1 106 BR (L) -- (3.9) SaO2 (%) 97 76 HR (/min) 131 164 100 Dyspnea 0.5 7 Legs 0 7 “Can’t do anymore … breathing and my legs.”
ILD / (?) Transplant Candidate 180 VO2max predicted HRmax predicted 2 140 Heart Rate (/min) VO2 (L/min) Wmax predicted 1 VO2max predicted 100 60 0 0 1 2 0 60 120 180 Workrate (W) VO2 (L/min)
ILD / (?) Transplant Candidate 70 R = 1 2 60 VE / VO2VE / VCO2 VCO2 (L/min) VO2max predicted VO2max predicted 1 50 40 0 2 0 1 2 0 1 VO2 (L/min) VO2 (L/min)
ILD / (?) Transplant Candidate 80 3 60 FEV1 x 35 VC 60 2 35 f (/min) VT (L) 40 40 VE (L/min) 1 20 FEV1 x 35 0 20 0 0 1 2 0 20 40 60 80 VCO2 (L/min) VE (L/min)
100 90 VO2max predicted SaO2 (%) 80 70 0 1 2 VO2 (L/min) ILD / (?) Transplant Candidate 50 40 30 PETCO2 (mmHg) VO2max predicted 20 10 0 1 2 VO2 (L/min)
ILD / (?) Transplant Candidate End-Exercise Measurements RA TestO2 Test%Change SaO2 (%) 76 92 + 21 HR (/min) 164 158 - 4 (100% pred) (96% pred) Wmax (watts) 50 75 + 50 (29% pred) (44% pred) Dyspnea 7 7 Legs 7 5 RA Test: “Can’t do anymore … breathing and my legs.” O2 Test: “My breathing gave out.”
Room Air O2 Room Air O2 ILD / (?) Transplant Candidate 100 180 HRmax predicted 90 140 SaO2 (%) Wmax predicted Heart Rate ( /min) Wmax predicted 80 100 70 60 0 60 120 180 0 60 120 180 Workrate (W) Workrate (W)
Interpretation physiologically maximal study with profound exercise limitation peak VO2 44% predicted VO2/kg = 10.8 ml/kg/min absent ventilatory reserve, significant arterial oxygen desaturation, ventilatory inefficiency, rapid/shallow breathing pattern abnormal cardiovascular responses improved performance [but not normalization] with supplemental oxygen ILD / (?) Transplant Candidate
Cardiopulmonary Exercise Testing The Bottom Line … • important to focus on the reason(s) for testing • ensures a correct and meaningful interpretation • multitude of graphical and numerical results, and an over-dependence on complicated algorithms contributes to confusion • focus on cardinal measurements and relationships • no single finding or measurement is diagnostic of any specific disease entity • CPET is never ordered, nor should it be interpreted in isolation