Download
1 / 27
270 likes | 271 Vues
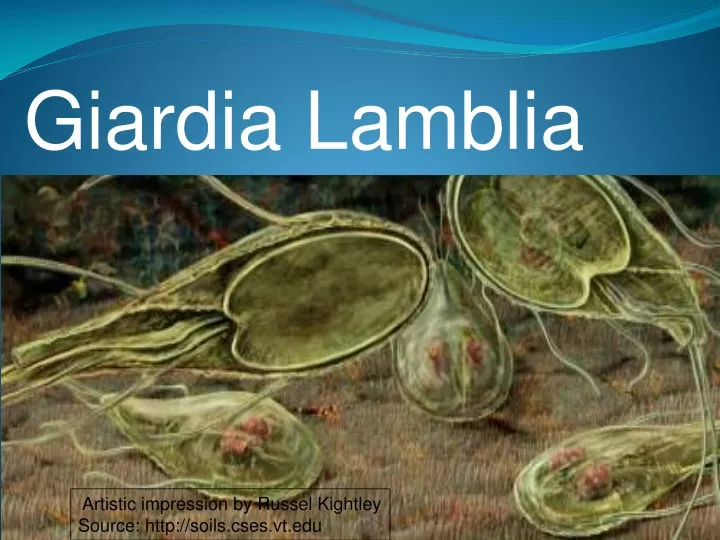
This is an artistic impression of Giardia Lamblia, a flagellated protozoan that infects the duodenum and small intestine. It can cause symptoms ranging from asymptomatic colonization to acute or chronic diarrhea and malabsorption. The artwork depicts the morphology and life cycle of Giardia.

E N D
Giardia Lamblia Artistic impression by Russel Kightley Source: http://soils.cses.vt.edu
Giardia • Giardia lambliais a flagellated protozoan that infects the duodenum and small intestine. • range from asymptomatic colonization to acute or chronic diarrhea and malabsorption. • more prevalent in children • Belongs to genus-Giardia-order-diplomonadida • Synonym- Giardia intestinalis ,lamblia intestinalis
HISTORY • First seen by Leeuwenhoek –(1681) while examining his own stool • Alexeieff-1914
EPIDEMIOLOGY • usually occurs sporadically • major reservoir for spread :water contaminated with Giardia cysts • Giardia cysts are relatively resistant to chlorination and to ultraviolet light irradiation • Boiling is effective for inactivating cysts. • Geographical distribution-world wide • Human milk contains glycoconjugates and secretory IgA antibodies that may provide protection to nursing infants.
Transmission -Water sports, surface contamination. Watershed contamination • Habitat - • -duodenum and upper part of jejunum of man
morphology • Exists in two phases-trophozoite and cyst form • Trophozoite form-when viewed flat-appears like tennis or badminton racket-when viewed side –on-resembles –spit pear • Size-14µm long • Anterior end is broad and rounded-posterior end tapers • Is bilaterally symmetrical & all organs are paired
Tear drop shaped • 2 adhesive discs, • 2 median bodies, • 2 nuclei • 4 pairs of flagella
CYST–is fully formed cyst –oval in shape =12µm long 7µm broad • The axostyles lie –more or less diagonally-form sort of dividing line • There are four nuclei –remain clustered at • one end • An acid environment-often cause parasite to encyst
four pairs flagellae a flat ventral surface sucking or adhesive disk 8 to 12 mm long and 7 to 10 mm wide convex dorsal surface Source: http://soils.cses.vt.edu
LIFE CYCLE life cycle of G. lamblia is composed of 2 stages: • trophozoites • cysts
In tropozoite stage • Parasite multiplies(intestine of man –binary fission) • when unfavourable condition in duodenum(encystment occur during encystment cells then divide into two within the cyst infection to man is brought by ingestion of cyst
Trophozoites : Lives in duodenum, jejenum and upper ileum They come in close contact to the mucosal, but do not invade the host. Adhesive disc fits over surface of epithelial cell The flagella act as a pump to move nutrients away from the microvilla and hold the adhesive disc near the mucosa. Rapid division to produce large numbers quickly
Pathogenesis and Immune response (1) • The production of diarrhea, and occasionally malabsorption, is the result of a complex interaction of Giardia with the host, • Infection occurs after oral ingestion of as few as 10 to 25 cysts. • After excystation, trophozoites colonize and multiply in the upper small bowel • Adherence of G. lamblia in the human gut may be via the disc • but may also involve specific receptor-ligand interactions
Pathogenesis and Immune response (2) Several pathogenic mechanisms have been postulated Disruption of the brush border Mucosal invasion Elaboration of an enterotoxin Stimulation of an inflammatory infiltration leading to fluid and electrolyte secretion and occasionally to villous changes
Ventral sucking disc Source: Gallery of histology Woods and Ellis2000 TEM micrograph showing the method of attachment to the duodenal wall.
Immune Response Partially protective immunity may develop to Giardia Immune response involves both cellular and humoral immunity Ig A, serum Ig G and Ig M are detected in patients: role of Ig A is not completely understood, probably inhibits trophozoite attachment IgA deficiency lead to chronic giardiasis Cell mediated immune response may also play a role Human milk may also play a role in protection of the host against Giardia : Free fatty acids and IgA antibodies
CLINICAL MANIFESTATIONS • incubation period :1–2 wk • clinical manifestations :asymptomatic . acute infectious diarrhea, chronic diarrhea with failure to thrive and abdominal pain or cramping. • Symptomatic infections occur more frequently in children than in adults. • Most symptomatic patients : acute diarrhea. low-grade fever, nausea, and anorexia; • intermittent or more protracted course characterized by diarrhea, abdominal distention and cramps, bloating, malaise, flatulence, nausea, anorexia, and weight loss develops
CLINICAL MANIFESTATIONS • stools may be profuse and watery and later become greasy and foul smelling • Stools do not contain blood, mucus, or fecal leukocytes • Varying degrees of malabsorption may occur.
Abnormal stool patterns may alternate with periods of constipation and normal bowel movements. • Malabsorption of sugars, fats, and fat-soluble vitamins has been well documented and may be responsible for substantial weight loss. • Giardiasis has been associated with growth stunting and repeated Giardia infections with a decrease in cognitive function in children in endemic areas.
Giardiasis should be considered in young children in child care or in any person who has had contact with an index case or a history of recent travel to an endemic area who has persistent diarrhea, intermittent diarrhea and constipation, malabsorption, crampy abdominal pain and bloating, failure to thrive, or weight loss
DIAGNOSIS • established by microscopy documentation of trophozoites or cysts in stool specimens, • 3 stool specimens are required to achieve a sensitivity of >90%. • Stool enzyme immunoassay (EIA) or direct fluorescent antibody tests are more sensitive • aspiration or biopsy of the duodenum or upper jejunum -Enterotest
Enterotest • Uses a coiled thread inside small weighted gelatin capsule • Swallowed after attaching the free end of the thread to cheek • Capsule passes through stomach to duodenum • After 2 hours, thread is withdrawn ,placed in saline • Centrifuged deposit of saline is examined for giardia
TREATMENT • should receive therapy : acute diarrhea failure to thrive exhibit malabsorption
Treatement • Metronidazole (250mg TID -5 days) • Trimidazole(2gms OD) • Furozolidone(100mg QID)-7-10 -days
PREVENTION • Handwashing • purify public water supplies adequately include chlorination and filtration. • Travelers to endemic areas are advised to avoid uncooked foods that might have been grown, washed, or prepared with water that was potentially contaminated. • Purification of drinking water can be achieved by a filter or by brisk boiling of water for at least 1 min