Download
1 / 1
10 likes | 205 Vues
No. 022. Radial Artery Based Free Forearm Flap in Urethral Reconstruction. Shrawan K Singh , Arup K Mandal , Gautam Biswas , Uttam K Mete, Santosh Kumar, Mayank Agarwal , Ravimohan Mavuduru

E N D
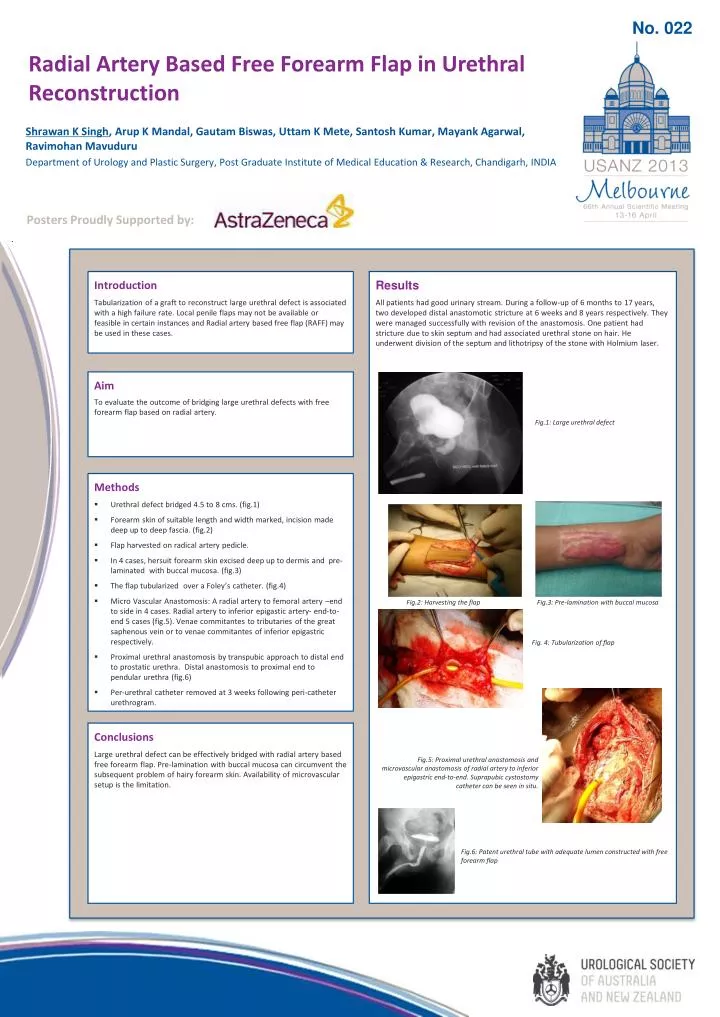
No. 022 Radial Artery Based Free Forearm Flap in Urethral Reconstruction Shrawan K Singh, Arup K Mandal, GautamBiswas, Uttam K Mete, Santosh Kumar, MayankAgarwal, RavimohanMavuduru Department of Urology and Plastic Surgery, Post Graduate Institute of Medical Education & Research, Chandigarh, INDIA Posters Proudly Supported by: Results All patients had good urinary stream. During a follow-up of 6 months to 17 years, two developed distal anastomotic stricture at 6 weeks and 8 years respectively. They were managed successfully with revision of the anastomosis. One patient had stricture due to skin septum and had associated urethral stone on hair. He underwent division of the septum and lithotripsy of the stone with Holmium laser. Introduction Tabularization of a graft to reconstruct large urethral defect is associated with a high failure rate. Local penile flaps may not be available or feasible in certain instances and Radial artery based free flap (RAFF) may be used in these cases. Aim To evaluate the outcome of bridging large urethral defects with free forearm flap based on radial artery. Fig.1: Large urethral defect • Methods • Urethral defect bridged 4.5 to 8 cms. (fig.1) • Forearm skin of suitable length and width marked, incision made deep up to deep fascia. (fig.2) • Flap harvested on radical artery pedicle. • In 4 cases, hersuit forearm skin excised deep up to dermis and pre-laminated with buccal mucosa. (fig.3) • The flap tubularized over a Foley’s catheter. (fig.4) • Micro Vascular Anastomosis: A radial artery to femoral artery –end to side in 4 cases. Radial artery to inferior epigastic artery- end-to-end 5 cases (fig.5). Venae commitantes to tributaries of the great saphenous vein or to venaecommitantes of inferior epigastric respectively. • Proximal urethral anastomosis by transpubic approach to distal end to prostatic urethra. Distal anastomosis to proximal end to pendular urethra (fig.6) • Per-urethral catheter removed at 3 weeks following peri-catheter urethrogram. Fig.2: Harvesting the flap Fig.3: Pre-lamination with buccal mucosa Fig. 4: Tubularization of flap Conclusions Large urethral defect can be effectively bridged with radial artery based free forearm flap. Pre-lamination with buccal mucosa can circumvent the subsequent problem of hairy forearm skin. Availability of microvascular setup is the limitation. Fig.5: Proximal urethral anastomosis and microvascularanastomosis of radial artery to inferior epigastric end-to-end. Suprapubiccystostomy catheter can be seen in situ. Fig.6: Patent urethral tube with adequate lumen constructed with free forearm flap