Download
1 / 64
730 likes | 1.34k Vues
The Respiratory System. Chapter 16 Part II. Lung Volumes and Capacities. Tidal volume – amount of air expired in each breath (quiet breathing) Vital capacity – max amount of air that can be forcefully exhaled after a max inhalation, equal to the sum of:

E N D
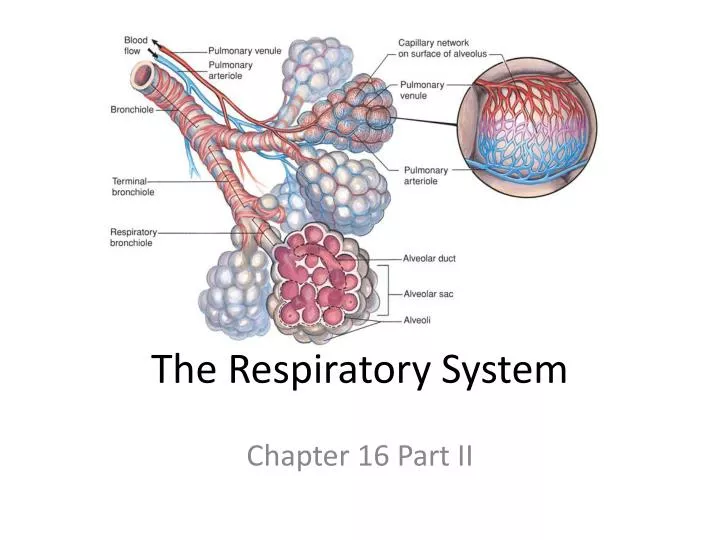
The Respiratory System Chapter 16 Part II
Lung Volumes and Capacities • Tidal volume – amount of air expired in each breath (quiet breathing) • Vital capacity – max amount of air that can be forcefully exhaled after a max inhalation, equal to the sum of: • inspiratory reserve vol + tidal vol + expiratory reserve vol • Functional residual capacity – sum of the residual volume and expiratory reserve volume • Total min vol = Tidal vol at rest X number of breaths/min (~6L/min) • During exercise tidal vol and number of breaths/min increase to produce a total min volume as high as 100 – 200 L/min • Anatomical dead space – conduction zone (no gas exchange occurs) • Lower O2 and higher CO2 concentrations than the external air
Restrictive and Obstructive Disorders • Restrictive Disorders – characterized by reduced vital capacity but with normal forced vital capacity • e.g. pulmonary fibrosis • Obstructive disorders – vital capacity is normal because lung tissue is not damaged • But expiration is more difficult and takes longer • Bronchoconstriction increases resistance to air flow • e.g. asthma
Obstructive Disorders – Asthma • Normal vital capacity but expiration is retarded • FEV1 = 1 sec forced expiratory volume test – measure rate of expiration
Pulmonary Disorders – Asthma • Frequently accompanied by dyspnea (shortness of breath) • Asthma – episodes of obstruction of air flow through bronchioles • Caused by inflammation, mucus secretion, and bronchoconstriction • Inflammation contributes to increased airway responsiveness to agents that promote bronchial constriction • Provoked by allergic reactions that release IgE, by exercise, by breathing cold, dry air, or by aspirin
Pulmonary Disorders - Emphysema • Chronic, progressive condition – destroys alveolar tissue, resulting in fewer and larger alveoli • Reduces surface area for gas exchange and ability of bronchioles to remain open during expiration • Air trapping: decrease gas exchange due to collapse of bronchiole during expiration • Commonly occurs in long-term smokers • Cigarette smoking stimulates release of inflammatory cytokines • Attract macrophages and leukocytes that secrete enzymes that destroy tissue
Emphysema Destroys Lung Tissue • Obstruction of lung tissue results in fewer and larger alveoli
Chronic Obstructive Pulmonary Disease • COPD – involves chronic inflammation accompanied by narrowing of airways and destruction of alveolar walls • Most people with COPD are smokers • Fifth leading cause of death
Pulmonary Fibrosis • Sometimes lung damage leads to pulmonary fibrosis instead of emphysema • Characterized by accumulation of fibrous connective tissue • Occurs from inhalation of particles <6m in size, such as in black lung disease (anthracosis) from coal dust
Gas Exchange in the Lungs • Partial pressure of gases • Partial pressure: pressure that a particular gas in a mixture exerts independently • Dalton’s Law – total pressure of a gas mixture (air) is equal to the sum of partial pressures of each gas in the mixture • Atmospheric pressure at sea level is 760 mm Hg • PATM = PN2 + PO2 + PCO2 + PH2O = 760 mm Hg • PO2 (21%) + PN2 (78%) = 99% of 760 mm Hg • Inspired air contains variable amount of moisture • When reaches respiratory zone saturated = 100% humidity
Effect of Altitude on Partial PO2 • With increasing altitude total atm pressure and partial pressure of the gases decrease • Below sea level total pressure increases by 1 atm for every 33 feet • At 33 feet pressure equals 2 X 760
Gas Exchange in Lungs – Inspired Air - Alveolar Air • Driven by differences in partial pressures of gases between alveoli and capillaries • As air enters the alveoli its O2 content decreases, CO2 content increases, and air is saturated with water vapor
Gas Exchange in Lungs • Facilitated by enormous surface area of alveoli, short diffusion distance between alveolar air and capillaries, and tremendous density of capillaries • Quickly help to bring O2 and CO2 in the blood and air into equilibrium
Partial Pressures of Gases in Blood • When blood and alveolar air are at equilibrium the amount of O2 in blood reaches a maximum value • Henry’s Law says that this value depends on solubility of O2 in blood (a constant), temperature of blood (a constant), and partial pressure of O2 • So the amount of O2 dissolved in blood depends directly on its partial pressure (PO2), which varies with altitude
Blood PO2 and PCO2 Measurements • Provide good index of lung function • At normal arterial blood has about PO2= 100mmHg • PO2 = 40mmHg in systemic veins • PCO2 = 46mmHg in systemic veins
Pulmonary Circulation • Rate of blood flow through pulmonary circuit equals flow through systemic circulation • But is pumped at lower pressure (about 15 mm Hg) • Pulmonary vascular resistance is low • Low pressure produces less net filtration than in systemic capillaries • Avoids pulmonary edema • Pulmonary arterioles constrict where alveolar PO2 is low and dilate where high • This matches ventilation to perfusion (blood flow)
Lung Ventilation/Perfusion(Blood Flow) Ratios • Normally, alveoli at apex of lungs are underperfused and overventilated • Alveoli at base are overperfused and underventilated
Disorders Caused by High Partial Pressures of Gases • Total atmospheric pressure increases by an atmosphere for every 10m below sea level • At depth, increased O2 and N2 can be dangerous to body • Breathing 100% O2 at < 2 atmospheres can be tolerated for few hrs • O2 toxicity can develop rapidly at > 2 atmospheres • Probably because of oxidation damage
Disorders Caused by High Partial Pressures of Gases • At sea level, nitrogen is physiologically inert • It dissolves slowly in blood • Under hyperbaric conditions takes more than hour for dangerous amounts to accumulate • Nitrogen narcosisresembles alcohol intoxication • Amount of nitrogen dissolved in blood as diver ascends decreases due to decrease in PN2 • If ascent is too rapid, decompression sicknessoccurs as bubbles of nitrogen gas form in tissues and enter blood, blocking small blood vessels and producing “bends”
Regulation of Breathing • Respiratory muscles controlled by 2 major descending pathways • One controls voluntary breathing • Another controls involuntary breathing • Unconscious rhythmic control of breathing • influenced by sensory feedback from receptors sensitive to • PCO2, pH, and PO2 of arterial blood
Brain Stem Respiratory Centers • Rhythmicity center in medulla oblongata – generates automatic • Consists of inspiratory neurons that drive inspiration • and expiratory neuronsthat inhibit inspiratory neurons • Their activity varies in a reciprocal way and may be due to pacemaker neurons
Brain Stem Respiratory Centers • Inspiratory neurons stimulate spinal motor neurons that innervate respiratory muscles • Expiration is passive and occurs when inspiratory neurons are inhibited • Activities of medullary rhythmicity center are influenced by centers in pons • Apneustic centerpromotes inspiration by stimulating inspiratory neurons in medulla • Pneumotaxic centerantagonizes apneustic center, inhibiting inspiration
Chemoreceptors • Automatic breathing – influenced by activity of chemoreceptors • monitor blood PCO2, PO2, and pH • Central chemoreceptorsare in medulla • Peripheral chemoreceptorsare in large arteries near heart (aortic bodies) and in carotids (carotid bodies)
Effects of Blood PCO2 and pH on Ventilation • Chemoreceptors modify ventilation to maintain normal CO2, O2, and pH levels • PCO2 is most crucial because of its effects on blood pH • H2O + CO2 H2CO3 H+ + HCO3- • H2O + CO2 H2CO3 • H2CO3 H+ + HCO3- • Hyperventilation causes low CO2 (hypocapnia) • Hypoventilation causes high CO2 (hypercapnia)
Effects of Blood PCO2 and pH on Ventilation • Brain chemoreceptors are responsible for greatest effects on ventilation • H+ can't cross BBB but CO2 can, which is why it is monitored and has greatest effects • Rate and depth of ventilation adjusted to maintain arterial PCO2 of ~40 mm Hg • Peripheral chemoreceptors do not respond to PCO2, only to H+ levels
Effects of Blood PCO2 and pH on Ventilation • Rise in blood CO2 increases [H+] • lowers pH of CSF • thereby stimulates chemoreceptor neurons in the medulla oblongata • .
Effects of Blood PO2 on Ventilation • Hypoxemia – low blood PO2 () has little effect on ventilation • Does influence chemoreceptor sensitivity to PCO2 • PO2 has to fall to about half normal before ventilation is significantly affected • Emphysema blunts chemoreceptor response to PCO2 • Oftentimes ventilation is stimulated by hypoxic driverather than PCO2
Effects of Pulmonary Receptors on Ventilation • Lungs have receptors that influence brain respiratory control centers via sensory fibers in vagus • Unmyelinated C fibersare stimulated by noxious substances such as capsaicin • Causes apnea followed by rapid, shallow breathing • Irritant receptorsare rapidly adapting; respond to smoke, smog, and particulates, causes cough • Hering-Breuer reflex– mediated by stretch receptors activated during inspiration • Inhibits respiratory centers to prevent overinflation of lungs
The Loading and Unloading Reactions • Loading reaction – deoxyhemoglobin (reduced hemoglobin) and oxygen combine to form oxyhemoglobin • Occurs in the lungs • Unloading reaction – oxyhemoglobin dissociates to yield deoxyhemoglobin and free oxygen molecules • Occurs in the systemic capillaries
Hemoglobin (Hb) and O2 Transport • Hb has 4 globin polypeptide chains • 4 heme groups that bind O2 • Each heme has a ferrous ion that can bind one molecule of oxygen • each Hb can carry 4 O2 • 280 million hemoglobin molecules per RBC • Each can carry over a billion oxygen molecules
Hemoglobin (Hb) and O2 Transport • Normal heme contains Fe2+ - can share electrons and bond with oxygen (oxyhemoglobin) • loads with O2 to form oxyhemoglobin in pulmonary capillaries • Deoxyhemoglobin (reduced hemoglobin) – oxyhemoglobin dissociates to release oxygen • Unloading in tissues • Affinity of Hb for O2 changes with a number of physiological variables
Hemoglobin (Hb) and O2 Transport • Most O2 in blood is bound to Hb inside RBCs as oxyhemoglobin • Each RBC has about 280 million molecules of Hb • Hb greatly increases O2 carrying capacity of blood
Hemoglobin (Hb) and O2 Transport • Methemoglobin– contains oxidized ferric iron (Fe3+) • Lacks electron to bind with O2 • Blood normally contains a small amount • Carboxyhemoglobin–heme combined with carbon monoxide • Carbon monoxide (CO) bond 210 times stronger than oxygen bond • CO poisoning heme cannot bind O2
Hemoglobin (Hb) and O2 Transport • O2-carrying capacity of blood depends on its Hb levels • Anemia, Hb levels are below normal • Polycythemia, Hb levels are above normal • Hb production controlled by erythropoietin (EPO) • Production stimulated by low PO2 in kidneys • Hb levels in men are higher because androgens promote RBC production
Hemoglobin (Hb) and O2 Transport • High PO2 of lungs favors loading • Low PO2 in tissues favors unloading • Ideally, Hb-O2 affinity should allow maximum loading in lungs and unloading in tissues
Oxyhemoglobin Dissociation Curve • Gives % of Hb sites that have bound O2 at different PO2 • Reflects loading and unloading of O2 • Differences in % saturation in lungs and tissues • Steep part of curve, small changes in PO2 cause big changes in % saturation
Oxyhemoglobin Dissociation Curve • Affected by changes in Hb-O2 affinity due to pH and temperature • Affinity decreases when pH decreases (Bohr Effect) or temp increases • Occurs in tissues where temp, CO2 and acidity are high • Causes Hb-O2 curve to shift right and more unloading of O2
Effect of 2,3 DPG on O2 Transport • RBCs have no mitochondria so no aerobic respiration • 2,3-DPG: a byproduct of glycolysis in RBCs • Production is increased by low O2 levels • Causes Hb to have lower O2 affinity, shifting curve to right
Effect of 2,3 DPG on O2 Transport • Anemia – total blood Hb levels fall, causing each RBC to produce more DPG • Fetal hemoglobin(HbF) has 2 gamma-chains in place of beta-chains of HbA • HbF can’t bind DPG, causing it to have higher O2 affinity • Facilitates O2 transfer from mom to baby
Anemia • Production of 2,3-DPG inhibited by oxyhemoglobin so a reduction in RBC content of oxyhemoglobin increases DPG production • Lowers affinity of Hb for O2 higher proportion converted to deoxyhemoglobin by unloading of its O2
Sickle-cell Anemia • Affects 8-11% of African Americans • HbS has valine substituted for glutamic acid at 1 site on b chains • At low PO2, HbS crosslinks to form a “paracrystalline gel” inside RBCs • Makes RBCs less flexible and more fragile
Thalassemia • Affects primarily people of Mediterranean descent • Has decreased synthesis of alpha or beta chains • Increased synthesis of gamma chains
Muscle Myoglobin • Red pigment found exclusively in striated muscle • Slow-twitch skeletal and cardiac muscle fibers are rich in myoglobin • Has only one globin; binds only one O2 • Has higher affinity for O2 than Hb; is shifted to extreme left • Releases O2 only at low PO2 • Serves in O2 storage, particularly in heart during systole
CO2 Transport • CO2 transported in blood in three forms: • as dissolved CO2 (10%) in the plasma (CO2 ~21 times more soluble than O2 in water) • as carbaminohemoglobin (20%) attached to an amino acid in hemoglobin • asbicarbonate ion, HCO3-(70%) that accounts for most of the CO2 carried by blood • In RBCs carbonic anhydrasecatalyzes formation of H2CO3 from CO2 + H2O • Favored by the high PCO2 found in capillaries of systemic circulation
Chloride Shift • High CO2 levels in tissues causes the reaction: CO2 + H2O H2CO3 H+ + HCO3-to shift right in RBCs • Results in high H+ and HCO3- levels in RBCs • H+ is buffered by proteins • HCO3- diffuses down concentration and charge gradient into blood causing RBC to become more positive • So Cl- moves into RBC (chloride shift)
Carbon Dioxide Transport and the Chloride Shift • CO2 transported as • Dissolved CO2 gas • Carbaminohemoglobin • H2CO3 and HCO3- • When bicarbonate diffuses out of the RBCs • Cl- diffuses in to retain electrical neutrality • This exchange is the chloride shift