Download
1 / 48
490 likes | 517 Vues
MYOCARDIAL and PERICARDIAL DISEASES. Dilated cardiomyopathy: The most common form of cardiomyopathy, is characterized predominantly by left ventricular dilation and decreased left ventricular systolic function .

E N D
Dilated cardiomyopathy: The most common form of cardiomyopathy, is characterized predominantly by left ventricular dilation and decreased left ventricular systolic function . Hypertrophic cardiomyopathy : Increased ventricular myocardial wall thickness, normal or increased systolic function, and often, diastolic (relaxation) abnormalities . Restrictive cardio- myopathy: Nearly normal ventricular chamber size and wall thickness with preserved systolic function, but dramatically impaired diastolic function leading to elevated filling pressures and atrial enlargement. The extremely heterogeneous heart muscle diseases associated with structural remodeling and/or abnormalities of cardiac function (cardiomyopathy) are important causes of morbidity and mortality in the pediatric population.
DILATED CARDIOMYOPATHY(DCM) • The most common form of cardiomyopathy in children, • Cause of significant morbidity and mortality as well as a common indication for cardiac transplantation. • Unlike adult patients with DCM, ischemic etiologies are rare in children; • anomalous origin of the left coronary artery from the pulmonary artery, • premature coronary atherosclerosis (homozygous type II hypercholesterolemia) • coronary inflammatory diseases( Kawasaki disease). Annual incidence of DCM in children younger than 18 yr is 0.57 cases per 100,000 per year. Incidence is higher in males, African-Americans, and in infants less than 1 yr old. MOST COMMON ETIOLGY REMAINS IDIOPATHIC 50% of cases are genetic (usually autosomal dominant; some autosomal recessive or X-linked.
Pathogenesis: • The pathogenesis of ventricular dilatation and altered contractility varies depending on the underlying etiology;SYSTOLIC DYSFUNCTION + MYOCYTE INJURY common. • Genetic abnormalities of several components of cardiac muscle (sarcomere protein, cytoskeleton, proteins that bridge the contractile apparatus to the cytoskeleton) Autosomal dominant or X-linked inherited disorders • Viral myocarditis ,viral induced inflammatory injury result in myocardial damage ,ventricular enlargement and poor function. • Anthracycline cardiotoxicity (doxorubicin) causes acute inflammatory myocardial injury, more clasiccaly results in DCM.
Clinical Manifestations: • Palpitations, syncope,sudden death. • Nonspesific complaints: Irritability,lethargy, failure to thrive ,nausea,vomiting. • Signs of heartfailure: Respiratory symptoms ( tachypnea, cough,dypnea on exertion). • Hepatic enlargement, rales or wheezing. • Auscultation: gallop rhythm,tachycardia, murmurs of mitral and tricuspid (less commonly) insufficiency. • Presence of hypoglycaemia, acidosis, hypotonia or signs of liver dysfunction suggests an inborn errors of metabolism. • Neurologic or skelatal muscle deficits are associated with mitochondrial disorders or muscular dystrophies.
Labrotory Findings : • ECG: • atrial or ventricular hypertrophy , • nonspesfic T-wave abnormalities, • atrial or ventricular arryhmias • CHEST X RAY: • cardiomegly • pulmonary vascular prominence • pleural effusions • ECHO:diagnostic • LV enlargement • decreased ventricular contractility, • RV enlargement and depressed function. • ECHO DOPPLER: • pulmonary hypertension • mitral regurgitation
Additional testing should include: complete blood count, renal and liver function tests, creatine phosphokinase, cardiac troponin I, lactate, plasma amino acids, urine organic acids, and acylcarnitine profile. • Additional genetic and enzymatic testingmay be useful . • Cardiac catheterization and endomyocardial biopsy are not routine but may be useful in patients with acute DCM. Biopsy samples can be examined histologically for the presence of mononuclear cell infiltrates, myocardial damage, storage abnormalities, and for evidence of infection. • It is considered standard of care to screen 1st-degree family members utilizing echocardiography and electrocardiogram (ECG) in idiopathic and familial cases of DCM.
Prognosis&Management • DCM is the most common cause for cardiac transplantation in pediatric and adult studies. • The therapeutic approach careful assessment to uncover possible treatable etiologies, screening of family member, rigorous pharmacologic therapy. • Decongestive therapymay improve symptoms of heart failure, prolong survival, and occasionally results in complete resolution of dysfunction. • Diuretics and ACE inhibitors. • Digitalis and angiotensin receptor blockers. • β-Adrenergic blockade with carvedilol or metoprolol is often used in patients with chronic heart failure. • In patients presenting with extreme degrees of heart failure or circulatory collapseintravenous inotropes and diuretics, mechanic ventilatorysupport,mechanicalcirculatory support, extracorporeal membrane oxygenation (ECMO), and ultimately cardiac transplantation. • In patients with DCM and atrial or ventricular arrhythmias, specifc antiarrhythmic therapy should be used.
HYPERTROPHIC CARDIOMYOPATHY(HCM) • Potentially life-threatening form of cardiomyopathy. • The causes of HCM are heterogeneous: • Inborn errors of metabolism • Neuromuscular disorders • Syndromic conditions, and genetic abnormalities of the structural components of the cardiomyocyte. • Both the age of onset and associated features are helpful in identifying the underlying etiology.
Pathogenesis: • Presence of increased left ventricular wall thickness in the absence of structural heart disease or hypertension. • Interventricular septum is disproportionately involved, leading to the previous designation of idiopathic hypertrophic subaortic stenosis (current term of asymmetric septal hypertrophy.) • Although the left ventricle is predominantly affected, the right ventricle may be involved, particularly in infancy. • Mitral valve can demonstrate systolic anterior motion and mitral insufficiency. Left ventricular outflow tract obstruction occurs in 25% of patients, and may in part be secondary to the abnormal position of the mitral valve as well as the obstructing subaortic hypertrophic cardiac muscle. • The cardiac myofibrils and myofilaments demonstrate disarray and myocardial fibrosis. • Systolic pump function is preserved or even hyperdynamic, though systolic dysfunction may occur late. • Outflow tract obstruction with or without mitral insufficiency may be provoked by physiologic manipulations (positional changes, and physical activity). • Hypertrophic and fibrosed cardiac muscle demonstrates relaxation abnormalities (diminished compliance) and left ventricular filling may be impaired (diastolic dysfunction).
Clinical Manfestations: • Many patient are asymptomatic.%50 cases present with a heart murmur or during screening when other family member has been diagnosed with heart HCM. • Palpitations, chest pain, easy fatiguability, dyspnea, dizziness and syncope. • Sudden death is well recognised but uncommon manifestation, often occurs during physical exertion. • Abnormal peripheral pulses (hyperdynamic or diminished), • Systolic ejection murmur in the aortic region. • Apical murmur of mitral insufficiency.
Labrotory Findings: • ECG: • Left ventricular hypertrophy (S wave in V1 + R wave in V5 or V6≥ 35 mm R wave > 11 mm in aVL ST segment and T-wave abnormalities, • Intraventricular conduction delay • CHEST X RAY: • Normal or mildly increased heart size with a prominent left ventricle • ECHO:diagnostic • Concentric LV hypertrophy • Asymmetric septalhypertrophy ECHO DOPPLER: • Diastolic dysfunction • Additional diagnostic studies include metabolic testing, genetic testing for speci c syndromes, or genetic testing for mutations in genes known to cause isolated HCM
Prognosis&Management: • Children under 1 yr of age or with inborn errors of metabolism or malformation syndromes or those with a mixed HCM/DCM have a signifcantlypoorer prognosis. • Competitive sports and strenuous physical activity should be pro- hibited. • β-adrenergic blocking agents (propranolol, atenolol) or calcium channel blocking agents (verapamil) may be useful in diminishing ventricular outflow tract obstruction, modifying ventricular hypertrophy, and improving ventricular filling. Although significant symptomatic improvement occurs in some patients, the risk for development of heart failure or sudden death has not been lessened. • In patients with atrial or ventricular arrhythmias, specific antiarrhythmic therapy should be used. • First-degree relatives of patients identified as having HCM should be screened with electrocardiography and echocardiography.
RESTRICTIVE CARDIOMYOPATHY (RCM) • Accounts for <5% of cardiomyopathy cases. • Incidence increases with age, and is more common in females. • Infiltrative myocardial causes and storage disorders frequently result in associated left ventricular hypertrophy and may represent HCM with restrictive physiology. • Nonininfiltrativecauses include mutations in genes encoding sarcomeric or cytoskeletal proteins. • Majority are considered idiopathic.
Pathogenesis: • Normal ventricular wall dimensions • Normal myocardial wall thickness • Preserved systolic function • Dramatic atrial diletation as a result of the abnormal myocardial compliance and high ventricular diastolic pressure.
Clinical Manifestations: • Abnormal vetricular filling (diastolic heart failure); edema,hepatomegaly, ascites. • Elevation of left-sided filling pressures; dypnea, cough,pulmonary edema. • With activity chest pain ,shortness of breath,syncope-near syncope or even sudden death. • Pulmonary hypertension and pulmonary vascular disease develop and may progress rapidly. Pronounced pulmonary component of the second heart sound are present. • Heart murmurs are typically absent, but a gallop rhythm may be prominent.
Labrotory Findings: • ECG: Prominent p waves with normal QRS voltages Nonspesific ST and T-wave changes RVH (in patients who develop PHT) (r wave tall in v1 v2) • CHEST X RAY: • Normal or prominent atrial shadow and pulmonary vascular redistribution ECHO: diagnostic • Normal sized ventricles with preserved systolic function • Dramatic enlargement of atria ECHO DOPPLER: • Abnormal filling parameters • Differential diagnosis from constrictive pericarditis is critical (can be treated surgically). • MRI may be necessary to demonstrate the thickened or calcifed pericardium often present in constrictive pericardial disease.
Prognosis and Management • Pharmacologic treatment :limited use • Prognosis :poor ,progressive clinical deterioration. • When signs of heart failure exist, use of diuretics can result in clinical improvement. • Dramatic atrial enlargementpredisposedto atrial tachyarrhythmias and thromboemboli.Antiarrhythmic agents+ anticoagulation with platelet inhibitors or Coumadin is indicated. • Cardiac transplantation is the treatment of choice,andthe results are excellent in patients without pulmonary hypertension, pulmonary vascular disease, or severe congestive heart failure.
MYOCARDITIS • Acute or chronic inflammation of the myocardium by inflammatory cell infiltrates, myocyte necrosis, or myocytedegeneration. • May be caused by: INFECTIOUS,CONNECTIVE TISSUE,GRANULAMATOUS, TOXIC ,IDIOPATHIC,IMMUNE DISORDERS,HYPERSENSITIVITY REACTIONS. • Patients may be asymptomatic, have nonspecific prodromal symptoms, or present with overt congestive heart failure, compromising arrhythmias, or sudden death. • Viral infections are the most common etiology
Pathophisiology: • Myocardial inflammation, injury or necrosis fibrosis. • Cardiac enlargement+ diminished systolic function as a direct result of the myocardial damage. Typical signs of congestive heart failure occur and may progress rapidly to shock, atrial or ventricular arrhythmias, and sudden death. • Viral myocarditis may also become a chronic process with persistence of viral nucleic acid in the myocardium, and the perpetuation of chronic inflammation secondary to altered host immune response including activated T lymphocytes (cytotoxic and natural killer cells) and antibody-dependent cell mediated damage.
Some viral proteins share antigenic epitopes with host cells, resulting in autoimmune damage to the antigenically related myocyte. • Cytokines (TNF-α and IL-1) are inhibitors of myocyte response to adrenergic stimuli, result in diminished cardiac function. Final result of viral-associated inflammation can be DCM.
Clinical Manifestations • Previous viral respiratory tract infection or diarhhea present. • Signs and syptoms change according to age. • Neonates: Fever,fatigue,pallor, inability to feed, sudden death • Congestive heart failure signs in physical examination. • Older children: Previous viral respiratory tract infection or diarhhea (10-14 days ago) • Fever,pallor, decreased appetite, dypnea,chestpain,vomiting,abdominal pain ,syncope, cardiac arrest. • Physical examination: tachycardia (when resting and without fever),CHF signs,arrythmias.
Diagnosis: • ECG: sinus tachycardia, low voltage QRS, low voltage T wave or inverse T wave. • Wide Q,ST segment changes mimicking MI. • Tachy-bradyarrythmias (VT,SVT, AF,AV block)
Telecardiography: Normal or enlarged heart • Pulmonary congestion,pleuraleffusions,interstitial infiltrates.
Echo: Diminished ventricular systolic funtion • Cardiac chamber enlargement • Mitral insufficiency • Pericardial effusion
Cardiac MRI :presence and extent of edema, gadolinium-enhanced hyperemic capillary leak, myocyte necrosis, left ventricular dysfunction, pericardial effusion . • Endomyocardialbiopsy inflammatory cell infiltrates or myocyte damage + molecular viral analysis using PCR techniques. • Nonspecific tests (serum findings of myocardial damage):, creatine phosphokinase isoenzymes CK-MB, cardiac troponin I,AST levels. • Acute phase reactants: CRP, sedimentation
Differential Diagnosis: • Newborns: • Sepsis • Hypoxia • Hypoglycemia • Hypocalcemia • Congenital heart diseases • Idiopathic DCM • Coronary anomalies • Other children: • Idiopathic DCM • Coronary anomalies • Chronic tachycardia • Pericarditis
Treatment: • Primary therapy for acute myocarditis issupportive. • Bed rest, activity restrictions • Respiratory distress: O2 treatment. • Anticongestive treatment: Acutely, inotropic agents (milrinone), should be entertained but used with caution because of their proarrhythmic potential. • Diuretics (Furosemide), ACE inhibitors (captopril), ARBsare of use in patients with compensated congestive heart failure • Digoxin : controlled+half dose ( damaged myocardial cells). • If in extremis, mechanical ventilatorysupport+ mechanical circulatory support (ECMO) may be needed to stabilize the patient’s hemodynamic status and serve as a bridge to recovery or cardiac transplantation. • Signifcantatrial or ventricular arrhythmiasspecificantiarrhythmic agents (amiodarone) .
Immunomodulationcontroversial. • Intravenous immune globulin may have a role in the treatment of acute or fulminant myocarditis (effective in Kawasaki) • Corticosteroids have been reported to improve cardiac function, but the data are not convincing in children. (first 7 days may increase viral replication). • Relapse has been noted in patients receiving immunosuppression who have been weaned from support. • Ribavirin: May inhibit Coxackievirus replication when used acutely. (same effect with α,βIFN).
Prognosis: • Newborns poor, 75% mortality . • Thee prognosis is better for children and adolescents, although patients who have persistent evidence of DCM often progress to need for cardiac transplantation. • Recovery of ventricular function has been reported in 10-50% of patients, however.
The heart is enveloped in a bilayer membrane, the pericardium, which normally contains a small amount of serous fluid. • The pericardium is not vital to normal function of the heart, and primary diseases of the pericardium are uncommon. However, the pericardium may be a affected by a variety of conditions, manifestation of a systemic illness and can result in serious, even life-threatening, cardiac compromise.
ETIOLOGY OF PERICARDIAL DISEASE • CONGENITAL • Absence (partial, complete)CystsMulibreynanism (TRIM 37 gene mutation) Camptodactyly-arthropathy-coxavara-pericarditis syndrome (PRG4 • INFECTIOUS • Viral (coxsackievirus B, Epstein-Barr virus, influenza, adenovirus, parvovirus, HIV, mumps) • Bacterial (Haemophilusinfluenzae, streptococcus, pneumococcus, staphylococcus, meningococcus, mycoplasma, tularemia, listeria, leptospirosis, tuberculosis, Q-fever, salmonella) • Immune complex (meningococcus, H. influenzae) Fungal (actinomycosis, histoplasmosis)Parasitic (toxoplasmosis, echinococcosis)
NONINFECTIOUS • IdiopathicSystemic inflammatory diseases (acute rheumatic fever, juvenile idiopathic arthritis, systemic lupus erythematosus, mixed connective tissue disorders, systemic sclerosis, Kawasaki disease, Churg-Strauss syndrome, Behçet syndrome, sarcoidosis, familial Mediterranean fever and other recurrent fever syndromes, pancreatitis, granulomatosis with polyangiitis) • Metabolic (uremia, hypothyroidism, Gaucher disease, very-long- chain acyl-CoA dehydrogenase deficiency) • Traumatic (surgical, catheter, blunt) Lymphomas, leukemia, radiation therapy, Primary pericardial tumors
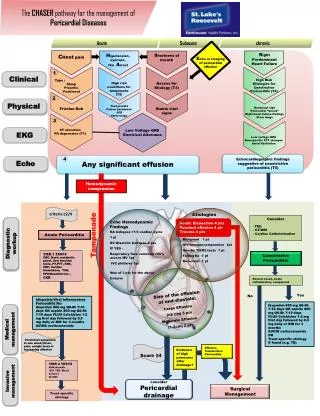
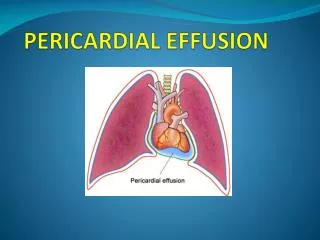
Pathogenesis: • When the amount of fluid in the nondistensible pericardial space becomes excessive, pressure in the pericardium increases ,resulting in impaired filling. • Small to moderate amounts of pericardial effusion can be well tolerated and clinically silent, once the noncompliant pericardium has been distended maximally, any further fluid accumulation causes abrupt impairment of cardiac filling and is termed cardiac tamponade. • When untreated, tamponade can lead to shock and death. • Withthedevelopment of pericardialtamponade, severalcompensatorymechanismsaretriggered: • systemicandpulmonaryvenousconstrictiontoimprovediastolicfilling, • an increase in SVR toraisefallingbloodpressure, and • tachycardiatoimprovecardiacoutput. • Pericardial effusions may be serous/transudative, exudative/purulent, fibrinous, or hemorrhagic.
Clinical Manifestations: • Chest pain(sharp/stabbing, positional, radiating, worse with inspiration, and relieved by sitting upright or prone). • Cough, fever, dyspnea, abdominal pain, and vomiting are nonspecific symptoms associated with pericarditis. • Distant heart sounds, tachycardia, narrow pulse pressure, jugular venous distention, and a pericardial friction rub provide clues to the diagnosis of acute pericarditis. • Cardiac tamponade is recognized by the excessive fall of systolic blood pressure (>10 mm Hg) with inspiration.
Diagnosis: • ECG:, low voltage QRS, low voltage T wave • Tachycardia and abnornormalitiesof the ST segments (elevation mimicing acute MI, PR segments(depression), and T waves(inversion).
Telecardiography: Normal without effusion or enlarged heart • Echo: identify size an location of pericardial fluid. Compression and collapse of the right atrium and/RV Abnormal diastolic filling during tamponade.
Differential Diagnosis: • Chest pain similar to that present in pericarditis can occur with lung diseases, especially pleuritis, and with gastroesophagealreflux. • Pain related to myocardial ischemia is usually more severe, more prolonged, and occurs with exercise, allowing distinction from pericarditis-induced pain.
Infectious pericarditis • Clinical course majority of these infections is mild and spontaneously resolving. • Enteroviruses, influenza, adenovirus, respiratory syncytial virus, and parvovirus. • Course is usually benign, symptomatic treatment with nonsteroidalantiinflammatory agents is often suffcient. • Large effusions and tamponade may require pericardiocentesis. • In up to 30%, there may be recurrences of pericarditis. Treatment and/or prevention of recurrences with colchicine improve symptoms -, avoid recurrences Patients with idiopathic recurrent pericarditis may also respond to treatment with anakinra. • Chronic or relapsing, surgical pericardiectomy or creation of a pericardial window may be necessary. • Echocardiography differentiates pericarditis from myocarditis, the latter diminished myocardial contractility or valvular dysfunction. Pericarditis and myocarditis may occur together in some cases of viral infection.
Purulant pericarditis (bacterial) much less common. More aggressive progression. • Tuberculous pericarditis is rare, causes constructive pericarditis.
Noninfectious Pericarditis • Systemic inflammatory diseases (autoimmune, rheumatologic, and connective tissue disorders) may involve the pericardium and result in serous pericardial effusions. • Pericardial inflammation may be a component of the type II hypersensitivity reaction seen in patients with acute rheumatic fever. It is associated with rheumatic valvulitis and responds quickly to antiinflammatoryagents including steroids. • Tamponadeis very uncommon. • Postpericardiotomysyndrome occurs in patients having undergone cardiac surgery and is characterized by fever, lethargy, anorexia, irritability, and chest/abdominal discomfort beginning 7-14 days postoperatively. Postpericardiotomysyndrome is effectively treated with aspirin, nonsteroidalantiinflammatory agents.
CONSTRICTIVE PERICARDITIS • Rarely, chronic pericardial inflammation can result in fibrosis, calcication, and thickening of the pericardium. • Pericardial scarring may lead to impaired cardiac distensibility and filling . • Constrictive pericarditis can occur following : • recurrent or chronic pericarditis, • cardiac surgery, or radiation to the mediastinum
Clinical Manifestations • Clinical manifestations of systemic venous hypertension predominate • Jugular venous distention, • peripheral edema, • Hepatomegaly, ascites • Tachycardia, • Hypotension, • Pulsusparadoxus. • Pericardial knock, rub, and distant heart sounds might be present on auscultation. • Abnormalities of liver function tests, hypoalbuminemia, hypoproteinemia, and lymphopenia may be present. • X-rays of the chest demonstrate calcifications of the pericardium.
Constrictive pericarditis may be difficult to distinguish clinically from restrictive cardiomyopathy as both conditions result in impaired myocardial filling. • Echocardiography may be helpful in distinguishing constrictive pericardial disease from restrictive cardiomyopathy, but magnetic resonance imaging and computed tomographic imaging are more sensitive in detecting abnormalities of the pericardium. • Although acute pericardial constriction is reported to respond to antiinflammatoryagents, the more typical chronic constrictive pericarditis will respond only to surgical pericardiectomy with extensive resection of the pericardium.