Download
1 / 135
1.35k likes | 1.36k Vues
This article explores the basic microbiology of dental infections, appropriate antibiotics, and discusses antibiotic misuse and prophylaxis in the treatment of dentoalveolar abscesses.

E N D
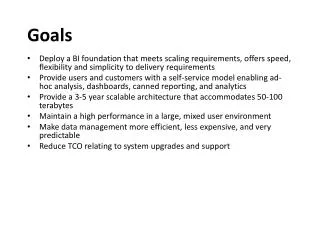
Goals • Review the basic microbiology of dental infections • Review the appropriate antibiotics for use in dental infection • Discuss antibiotic misuse and prophylaxis
The Dentoalveolar Abscess • Listed as the #5 or 6 leading cause of death in the 1600s in English records • In the early 20th century the mortality rate from dental infection was 10-40% • In the US acute dental infections account for 1 in 2600 hospital admissions • Periapical abscesses account for almost 50% of dental related ER visits in the US • 12% of antibiotics in the outpatient setting are given for odontogenic infections
What Pathogens Are We Dealing With? • Gram Positive? • Gram Negative? • Mixed Infection? • Aerobes? • Facultative? • Anaerobes?
Oral Cavity Organisms • More than 700 species • Aerobic as well as anaerobic • Anaerobic 10 – 100 times more common • Spirochetes, Candida, viruses
The Dentoalveolar Abscess • Polymicrobial infections • Facultative anaerobes such as Strep viridans and Strep anginosus groups • Strict anaerobes such as Prevotella and Fusobacterium • Anaerobes predominate • Treated by surgery to drain pus and eliminate the source of infection with antibiotics as an adjunct to limit the spread of severe infections
Recent Changes in Microbiology • Changes in identification of pathogens • Changes in nomenclature • Increased understanding of bacterial interactions
Gram Stain • Accurate for early diagnosis and treatment • Practical guide to antibiotic therapy • Inexpensive and available
Aerobic vs. Anaerobic • Aerobic bacteria - require oxygen • Microaerophilic bacteria - require lower than atmospheric concentration of O2 • Facultative anaerobes - can tolerate oxygen but grow better in an anaerobic environment • Strict anaerobes can only grow in the absence of O2
Why Molecular Techniques? • 60% of oral flora are uncultivable • Molecular biological techniques allow species identification by detection of bacterial genes • 16s rRNA or rDNA gene sequencing by molecular cloning • Proportionate amplification of DNA by Polymerase Chain Reaction (PCR) • Fast results • Has shown a higher prevalence of fastidious organisms such as Treponema species • Offers little information on antibiotic susceptability
Culture and Sensitivity • Takes 24-48 hours to obtain initial results, more time required for anaerobes or rare bacteria • Kirby-Bauer Agar Diffusion- most common • Tube dilution- used when concentration of antibiotic is necessary
When Are Cultures Necessary? • Serious infections (life threatening) • Infections that persist or recur in spite of treatment • Previous multiple antibiotic treatment • Immunocompromised patients • Osteomyelitis • Suspected actinomycosis
Culture and Sensitivity • Specimen acquisition and transport • Swabs • Aspirates • Biopsies • Secretions
Sensitivity Testing • Definitive antibiotic selection • Delayed results
Strep Viridans (Aerobic Streptococci) • S. anginosus • S. inetermedius • S. contellatus • S. mutans • S. sanguis • S. mitis • S. salivarius • S. vestibularis
The Strep Milleri Group • S. anginosus • S. intermedius • S. constellatus
Oral Anaerobic Streptococci • Old nomenclature: Peptococcus • New nomenclature: Peptostreptococcus • New and improved nomenclature: Anaerococcus
Oral Bacteroides Nomenclature Prevotella species: • P. melaninogenica • P. intermedia • P. oralis • P. buccae • P. loeschii • P. denticola • P. ruminicola • P. nigrescens (new)
Oral Bacteroides Nomenclature Porphyromonas species • P. asaccharolyticus • P. gingivalis • P. endodontalis • P. circumdentaria • P. salivarius
Odontogenic Infections • 300-700 species of which more than 50% cannot be cultured • Aerobic - anaerobic infections • Aerobes only (7%) • Mixed (60%) • Anaerobes only (33%) • Average isolates per specimen - 4 • Gram + Aerobic & Facultative Streptococci • Common pathogen and most numerous • Produce hyaluronidase and streptokinase
Major Pathogens of Orofacial Infections • Early infections Strep milleri group • Mature Infections - Strep viridans group Peptostreptococcus species Prevotella Species Fusobacterium Species
Progression of Odontogenic Infections • Initiated by aerobic organisms • Gain entrance to tissue • Aerobic bacteria cause cellulitis • Cause hypoxia and acidosis • Produce a favorable environment for anaerobes • Anaerobes follow • Tissue destruction leads to pus • Enzymes destroy antibiotics • Symbiosis between organisms leads to serious infections
Bacterial Interactions in Odontogenic Infections • Combinations of streptococci and anaerobes • Anaerobic dependence on other organisms • Anaerobic progression • Penicillinase release • Opsoinization interference (inhibit antibody attachment)
What Type of Antibiotic Should We Use? • Narrow Spectrum? • Broad Spectrum? • Bacteriostatic? • Bactericidal? • Designer Antibiotics?
The Ideal Antibiotic • Rapid onset of action • Specific for the pathogen • Does not disturb non-pathogens • No other side effects • Inexpensive
Choosing The Right Antibiotic • Is an antibiotic indicated? • Use empirical therapy routinely • Narrow spectrum • Avoid toxicity and side effects • Bactericidal vs bacteriostatic • Cost • Avoid allergies
Systemic Antibiotics Are Usually Not Needed For: • Chronic localized abscess • Minor vestibular abscess • Alveolar Osteitis (Dry socket) • Root canal sterilization • Mild pericoronitis
Basic Antibiotic Principals: • Hit hard, fast and early. Loading dose. • Use the right drug. • Use the right dose. Peak plasma level 4-5x MIC • Use the correct dosing schedule. Interval 4x plasma half-life • Use for the correct duration. Continue therapy for 2-3 days after resolution of infection
Penicillins • Still empiric drugs of choice for outpatient odontogenic infections because of: • Effectiveness • Side-effect profile • Cost
Penicillin Groups • Natural – Pen V and Pen G • First Generation – Nafcillin, Oxacillin, Cloxacillin, and Dicloxacillin • Second Generation – Ampicillin, Amoxicillin • Third Generation – Ticarcillin • Fourth Generation – Piperacillin
Adverse Reactions With Penicillins • Allergy: 3-5% (10% if previously taken) • Anaphylaxis: .004-.015% (10% these are fatal) • 75% fatal anaphylactic reactions in U.S!! • Only 70% deaths have hx of taking penicillin! • Most deaths after IV administration
Other Adverse Effects With Penicillins • Superinfections (candida) • Antibiotic associated colitis (AAC) • Blood dyscrasias: (granulocytopenia, anemia) • Interstitial nephritis
Penicillins • Natural penicillins • Pen VK and Pen G • Bactericidal (affects cell wall synthesis) • Spectrum: Oral strep, oral anaerobes, Actinomyces, Eikenella species • Resistant: Mostly staph (>80%), enteric species, B. fragilis • Excreted by kidneys
Penicillin VK • Potassium salt of penicillin V (1.7mEq K+/mil) • More water soluble, thus better absorbed • More resistant to gastric acid Dose: • 500 mg 4 times daily or up to 24 mil units/24 hr IV (Aqueous Pen G)
Semisynthetic Penicillins • All are bactericidal and inhibit cell wall synthesis • Penicillin: Procaine Pen G • Penicillinase resistant: cloxacillin, dicloxacillin, nafcillin, oxacillin, methicillin • Aminopenicillins • ampicillin, amoxicillin, cyclacillin, bacampacillin • Extended Spectrum • carbenicillin, ticarcillin, piperacillin, mezlocillin
Amino Penicillins:Amoxicillin • Stable in gastric acid • Does NOT penetrate CSF well • Excreted unchanged • Less effective against oral strep than Pen V • Most common cause of antibiotic associated colitis • Diarrhea in 10% of patients
Amoxicillin Spectrum Broader spectrum than Pen V Gram Positive • Alpha & beta hemolytic strep • Diplococcus pneumonia • Strep faecalis Gram negative • Many strains H. influenzae • Neisseria gonorrhea • E. Coli • Proteus mirabilis
Amoxicillin • Dose • 500 mg three times daily (T.I.D.) • 875mg BID (Amoxil) • 20-50mg per kg/day in children
Beta Lactamase Inhibitors • Beta lactamase is a bacterial enzyme that hydrolyzes the beta lactam ring • Clavulanic Acid • inhibits plasmid and chromosomal mediated beta Lactamases (including Staph, Haemophilus, Bacteroides) • Sulbactam • same spectrum as above • Tazobactam • penicillanic acid sulfone • poor activity against chromosomal B lactamases, good against plasmid B lactamases
Amoxicillin/Clavulanate (Augmentin) • Potassium salt of clavulanic acid (Beta-lactamase inhibitor) added • Dose: Same as amoxicillin, clavulanate dose does not go up as amoxicillin dose size goes up • Indications • Beta lactamase producing organisms • H. influenzae, S. aureus, E. Coli, Klebsiella • Adult dose:500-875 mg amoxicillin with 125 mg clavulanate potassium (TID to BID)
Piperacillin/Tazobactam (4th Generation) • Extended spectrum beta lactamase activity • Gram+ species, Neisseria, Haemophilus, Enterobacter • Excellent against anaerobes • Sufficient bone penetration • Good for severe intra-abdominal and soft tissue infections and as an alternative for severe head and neck infections Al-Nawas B, et al. J CraiomaxSurg, 36, 2008, 468
Carbapenems • Beta lactam antibiotics with wide spectrum of coverage and beta lactamase resistance • Coverage of Gram+, Gram-, and anaerobes • Not first line therapy for routine odontogenic infections but consider for multi-space infections or in cases of descending necrotizing mediastinitis
Carbapenems • Imipenem - • Cilastin added to decrease renal excretion • Seizures at high doses • Rare cross allegery with PCN • Meropenem • Ertapenem • Doripenem