Download
1 / 63
640 likes | 695 Vues
Applied Pathophysiology: A Conceptual Approach Chapter 3: Inflammation and Tissue Repair. Lines of Defense. First: Skin and mucous membranes Second: Inflammatory response Third: Immune response. Acute Inflammation. Triggered by tissue injury Goals of inflammation

E N D
Applied Pathophysiology:A Conceptual ApproachChapter 3: Inflammation and Tissue Repair
Lines of Defense • First: Skin and mucous membranes • Second: Inflammatory response • Third: Immune response
Acute Inflammation • Triggered by tissue injury • Goals of inflammation • Increase blood flow to site • Increase healing cells at site • Prepare for tissue repair
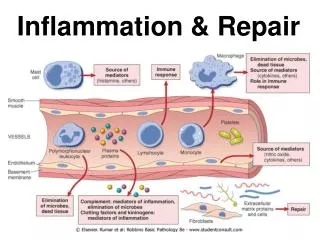
Vascular Response • Facilitated by chemical mediators • Induces vasodilation and increases capillary permeability • Objective is to get more blood flowing to the injured area
Inflammatory Mediators • Cell-derived • White blood cells • Platelets • Endothelial or damaged tissue cells • Plasma-derived • Complement system • Kinin system • Clotting system
Cellular Response • Chemotaxis • Cellular adherence • Cellular migration
Manifestations of Inflammation • Local manifestations include heat, incapacitation, pain, edema, redness • Systemic manifestations may include fever and increased circulating leukocytes and plasma proteins
Treatment of Inflammation • Reduce blood flow • Decrease swelling • Block the action of chemical mediators • Decrease pain
Healing and Tissue Repair • Inflammatory phase • Acute inflammatory response • Seal the wound • Proliferative phase • Clear the debris • Restore structural integrity • Remodeling phase • Restore functional integrity • Remodeling
Complications of Healing • Infection • Ulceration • Dehiscence • Keloids • Adhesions
Chronic Inflammation • Recurrent or persistent inflammation lasting several weeks or longer • Monocytes, macrophages, and lymphocytes more prominently involved • Formation of granulomas and scarring often occur
Application of the Concepts of Inflammation • Sinusitis • Burns • Rheumatoid arthritis (RA) • Gastritis • Pancreatitis • Inflammatory bowel disease (IBS)
Acute and Chronic Sinusitis • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
Acute SinusitisPathophysiology • Blockage of ostia and outflow of mucus due to allergy, viruses, or other irritants • Impaired clearance of mucus by cilia • Altered mucus quality or quantity • Cystic fibrosis
Acute SinusitisClinical Manifestations • Facial pain over sinus regions of face increasing with straining or bending down • Fever • Nasal congestion and/or excessive nasal discharge and postnasal drainage • Persistent cough • Fatigue
Acute SinusitisDiagnostic Criteria • Physical examination • General laboratory tests • Erythrocyte sedimentation rate (ESR) • C-reactive protein (CRP) test • White blood cell (WBC) count • Sinus radiographs
Acute Sinusitis Treatment • Pharmacologic • Antibiotics • Antihistamines • Decongestants • Nasal sprays • Surgical
Chronic Sinusitis Pathophysiology • Multifactorial • Environmental factors • Persistent infection • Allergens • Genetic factors • Metabolic abnormalities • Immune deficiencies • Disruption of mucociliary clearance
Chronic SinusitisClinical Manifestations • Nasal congestion • Nasal and postnasal discharge • Sore throat • Foul breath, unpleasant taste • Low-grade fever • Fatigue, anorexia • Chronic cough • Hyposmia (reduced ability to smell) • Facial fullness, discomfort, pain, and headache (with polyps)
Chronic SinusitisDiagnostic Criteria • Physical examination • Computed tomography (CT) scan
Chronic SinusitisTreatment • Pharmacologic • Glucocorticoids • Antibiotics • Nonpharmacologic • Nasal saline irrigation • Surgical
Burns • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
Burns Pathophysiology • Cause: direct contact with excessive heat or radiation, caustic chemicals, or electricity • Result: acute inflammatory response • Burn severity is correlated with exposure type and time
Burns Pathophysiology: Classification • Superficial partial-thickness • Deep partial-thickness • Full-thickness
Burns Clinical Manifestations • Superficial partial-thickness burns • Heat, swelling, pain, redness, loss of function • Deep partial-thickness burns • Blistering, redness, heat, pain, edema, serous exudate • Full-thickness burns • Redness, eschar, edema, exudate
Burns Diagnostic Criteria • Rule of nines
BurnsDiagnostic Criteria (cont’d) • American Burn Association has designated criteria for distinguishing minor, moderate, and major burns based on • Wound depth • Surface area • Required level of treatment
Burns Treatment • American Burn Association criteria • Remove source of injury and cool/rinse skin • Airway, breathing, circulation • Fluids, nutrition, antibiotics, analgesics • Wound management may include • Hydrotherapy • Skin grafting
Rheumatoid Arthritis (RA) • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
RA Pathophysiology • Chronic inflammation of synovial membranes and synovial hyperplasia • Etiology combines • Genetics • Triggering event • Autoimmunity
RA Pathophysiology (cont’d) • Remissions and exacerbations • Pannus formation • Cartilage erosion • Fibrosis • Ankylosis
RA Clinical Manifestations • Mild to debilitating • Symmetrical joints • Pain, stiffness • Redness, heat, swelling • Decreased mobility
RA Diagnostic Criteria • No definitive test • Increased likelihood with positive findings • Erythrocyte sedimentation rate (ESR) • C-reactive protein (CRP) • Rheumatoid factor (IgG) • Antinuclear antibodies (ANA)
RA Treatment • Pharmacologic: drugs that induce remission • Nonpharmacologic: • Rest/activity balance • Physical therapy exercises • Splints • Surgery
Acute and Chronic Gastritis • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
Acute Gastritis Pathophysiology • Ingestion of irritating substances and/or poor gastric perfusion results in acute inflammation of the gastric mucosa • Gastric epithelial cell necrosis • Gastric acid erodes underlying tissue
Acute Gastritis Clinical Manifestations • Mild to severe abdominal pain • Indigestion • Loss of appetite • Nausea • Vomiting • Hiccups
Acute Gastritis Diagnostic Criteria • History and physical examination • Endoscopic examination • Stool analysis (presence of blood in stool) • Complete blood count (anemia)
Acute Gastritis Treatment • Discontinue ingestion of irritating substance • Buffer or decrease production of gastric acid
Chronic Gastritis Pathophysiology • Chronic infection or autoimmune process leading to chronic inflammation • Infection with Helicobacter pylori bacterium • Gastric epithelial and mucosal cell atrophy • Gastric acid production impaired
Chronic Gastritis Clinical Manifestations • Dyspepsia • Loss of appetite • Vomiting • Anemia • Can be asymptomatic
Chronic Gastritis Diagnostic Criteria • Endoscopic examination • Biopsy of gastric tissue • Breath test • Blood test (protein antibodies)
Chronic Gastritis Treatment • Antibiotics for chronic infectious processes • Proton pump inhibitors or bismuth (antimicrobial and raise gastric pH) • Immunosuppressive drugs for autoimmune processes • Vitamin B12
Acute and Chronic Pancreatitis • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
Acute PancreatitisPathophysiology • Injury to • Acinar cells • Zymogen • Pancreatic duct • Protective digestive feedback mechanisms • Caused by • Duct blockage by gallstones • Excessive alcohol use
Acute PancreatitisPathophysiology (cont’d) • Acute pancreatitis as a result of gall stone obstruction
Acute PancreatitisClinical Manifestations • Upper abdominal pain • Sudden onset • Growing intensity • Dull, steady ache • Radiating to back • Nausea • Vomiting • Anorexia • Diarrhea
Acute PancreatitisDiagnostic Criteria • History and physical examination • Laboratory testing • Complete blood count, ESR, CRP • Serum amylase and lipase • Serum alkaline phosphatase • Total bilirubin • Aspartate aminotransferase (AST) • Alanine aminotransferase (ALT)
Acute PancreatitisTreatment • Intravenous hydration • Analgesics • Surgical removal of gallstones