Download
1 / 1
20 likes | 278 Vues
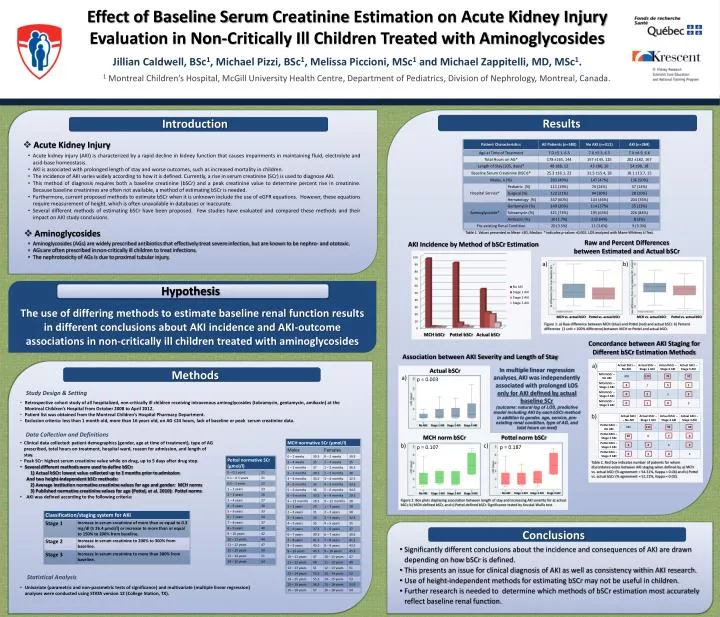
Effect of Baseline Serum Creatinine Estimation on Acute Kidney Injury Evaluation in Non-Critically Ill Children Treated with Aminoglycosides. Jillian Caldwell , BSc 1 , Michael Pizzi , BSc 1 , Melissa Piccioni , MSc 1 and Michael Zappitelli , MD, MSc 1 .

E N D
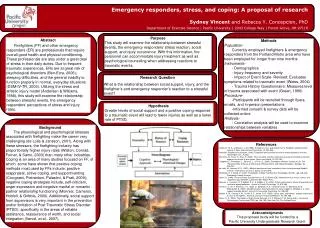
Effect of Baseline Serum Creatinine Estimation on Acute Kidney Injury Evaluation in Non-Critically Ill Children Treated with Aminoglycosides Jillian Caldwell, BSc1, Michael Pizzi, BSc1, Melissa Piccioni, MSc1 and Michael Zappitelli, MD, MSc1. 1 Montreal Children’s Hospital, McGill University Health Centre, Department of Pediatrics, Division of Nephrology, Montreal, Canada. Introduction Results Conclusions • Acute Kidney Injury • Acute kidney injury (AKI) is characterized by a rapid decline in kidney function that causes impairments in maintaining fluid, electrolyte and acid-base homeostasis. • AKI is associated with prolonged length of stay and worse outcomes, such as increased mortality in children. • The incidence of AKI varies widely according to how it is defined. Currently, a rise in serum creatinine (SCr) is used to diagnose AKI. • This method of diagnosis requires both a baseline creatinine (bSCr) and a peak creatinine value to determine percent rise in creatinine. Because baseline creatinines are often not available, a method of estimating bSCr is needed. • Furthermore, current proposed methods to estimate bSCrwhen it is unknown include the use of eGFR equations. However, these equations require measurement of height, which is often unavailable in databases or inaccurate. • Several different methods of estimating bSCr have been proposed. Few studies have evaluated and compared these methods and their impact on AKI study conclusions. • Aminoglycosides Table 1. Values presented as Mean ±SD, Median. * indicates p-values <0.001. LOS analyzed with Mann-Whitney U Test. Raw and Percent Differences between Estimated and Actual bSCr • Aminoglycosides (AGs) are widely prescribed antibiotics that effectively treat severe infection, but are known to be nephro- and ototoxic. • AGs are often prescribed in non-critically ill children to treat infections. • The nephrotoxicity of AGs is due to proximal tubular injury. AKI Incidence by Method of bSCr Estimation a) b) Hypothesis Methods MCH vs. actual bSCr Pottel vs. actual bSCr MCH vs. actual bSCr Pottel vs. actual bSCr The use of differing methods to estimate baseline renal function results in different conclusions about AKI incidence and AKI-outcome associations in non-critically ill children treated with aminoglycosides Figure 1: a) Raw difference between MCH (blue) and Pottel (red) and actual bSCr. b) Percent difference (1 unit = 100% difference) between MCH or Potteland actual bSCr. Concordance between AKI Staging for Different bSCr Estimation Methods Association between AKI Severity and Length of Stay a) In multiple linear regression analyses, AKI was independently associated with prolonged LOS only for AKI defined by actual baseline SCr (outcome: natural log of LOS, predictive model including AKI by each bSCr method in addition to gender, age, service, pre-existing renal condition, type of AG, and total hours on med) Actual bSCr a) p = 0.003 Study Design & Setting • Retrospective cohort study of all hospitalized, non-critically ill children receiving intravenous aminoglycosides (tobramycin, gentamycin, amikacin) at the Montreal Children’s Hospital from October 2008 to April 2012. • Patient list was obtained from the Montreal Children’s Hospital Pharmacy Department. • Exclusion criteria: less than 1 month old, more than 16 years old, on AG ≤24 hours, lack of baseline or peak serum creatinine data. b) Stage 1 AKI Stage 1 AKI Stage 1 AKI Stage 2 AKI Stage 2 AKI Stage 2 AKI Stage 3 AKI Stage 3 AKI Stage 3 AKI No AKI No AKI No AKI Data Collection and Definitions MCH norm bSCr Pottel norm bSCr • Clinical data collected: patient demographics (gender, age at time of treatment), type of AG prescribed, total hours on treatment, hospital ward, reason for admission, and length of stay. • Peak SCr: highest serum creatinine value while on drug, up to 5 days after drug stop. • Several different methods were used to define bSCr: 1) Actual bSCr: lowest value collected up to 3 months prior to admission And two height-independent bSCr methods: 2) Average institution normative creatinine values for age and gender: MCH norms 3) Published normative creatinine values for age (Pottel, et al. 2010): Pottel norms • AKI was defined according to the following criteria: b) c) p = 0.107 p = 0.187 MCH norm bSCr Table 2. Red box indicates number of patients for whom discordance exists between AKI staging when defined by a) MCH vs. actual bSCr(% agreement = 54.31%, Kappa = 0.04) and b) Pottelvs. actual bSCr (% agreement = 51.21%, Kappa = 0.02). Figure 2: Box plots displaying association between length of stay and increasing AKI severity for a) actual bSCr, b) MCH-defined bSCr, and c) Pottel-defined bSCr. Significance tested by Kruskal-Wallis test. • Significantly different conclusions about the incidence and consequences of AKI are drawn depending on how bSCr is defined. • This presents an issue for clinical diagnosis of AKI as well as consistency within AKI research. • Use of height-independent methods for estimating bSCr may not be useful in children. • Further research is needed to determine which methods of bSCr estimation most accurately reflect baseline renal function. Statistical Analysis • Univariate(parametric and non-parametric tests of significance) and multivariate (multiple linear regression) analyses were conducted using STATA version 12 (College Station, TX).