Download
1 / 39
440 likes | 852 Vues
Overview of Chronic Allograft Dysfunction (CAD). Prof. Dr. Nurul Islam MRCP(UK), FRCP(Edin) Consultant Nephrologist United Hospital, Dhaka. Introduction.

E N D
Overview of Chronic Allograft Dysfunction (CAD) Prof. Dr. Nurul Islam MRCP(UK), FRCP(Edin) Consultant Nephrologist United Hospital, Dhaka
Introduction • Over the last 2 decades incidence of acute rejection and one year graft survival has improved significantly with improved surgical techniques and use of new immunosuppressive agents including induction therapy • Long term graft and patients survival beyond 1 year post-transplant has not been consistent
Graft Survival following renal transplant in USA (1996-2006) 2 year survival 5 year survival 10 year survival 1 year survival Source: SRTR 2008
Major long-term risks of transplant recipient • Death from cardiovascular, malignant or infectious diseases • Chronic Allograft dysfunction (CAD) leading to ESRD
Causes of death in people with a functioning graft • Cancer is the most common cause of death in people who have functioning renal allograft
Chronic Allograft Dysfunction • CAD may be defined as progressive decline in renal function associated with histological changes in the graft • Clinically manifested as proteinuria, hypertension, slowly rising serum creatinine and falling GFR
Assessment of renal dysfunction • Longitudinal measurement of serum creatinine is not a very reliable indicator of assessing kidney function • GFR measurement by different method has its own biasness • Measurement of eGFR at 3, 6,12 months is the best alternative to predict CAD in the long run • Serum cystatin c is a reliable indicator
Risk factors for Chronic Allograft Dysfunction • Immunologic: - Cell mediated rejection - AMR - Sub-optimal immunosupression - Prior acute rejection andSCR - HLA mismatch - PRA/DSA • Non-immunologic: - Donor organ quality (age, sex, nephronmassliving vs deceased donor) - DGF/ ischemia-reperfusion injury / ATN - CNI nephrotoxicity • Infections: CMV, BK virus
Risk of Allograft Dysfunction.. cont • Recipient related factors: - Age - Hypertension - DM/PTDM - Hyperlipidaemia - Compliance - Recurrent disease • Urological complications
*Delayed graft function (DGF): major predictor of graft failure Quiroga I, et al. Nephrol Dial Transplant 2006
D/D of late allograft dysfunction Intrinsic renal disease • CAN • Chronic CNI toxicity • Late acute rejection / chronic AMR • recurrence of glomerular disease • BK virus nephropathy Vascular • Renal artery stenosis Urologic • Urinary tract obstruction • BK virus associated ureteric stenosis
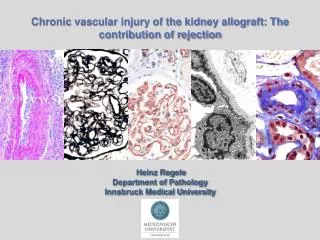
Chronic Allograft Nephropathy Pathologically all four compartments of the kidney are affected • Interstitial fibrosis • Tubular atrophy • Glomerulopathy • Concentric intimal thickening of the arteries and arterioles
Years after transplantation CNI Nephrotoxicity (%)
Anti-HLA antibody / DSA • Presence of anti-HLA antibody in the post-transplant period adversely affect the graft outcome • Antibody against class 1 HLA antigen is usually associated with acute AMR • Whereas Antibody against class 2 HLA antigen is associated with chronic AMR
•HLA antibody development within 1-year posttransplant markedly lowers allograft survival Lee PC, et al. Transplantation 2009
•Renal allograft biopsy (silver staining) •Evidence of “double contours” in capillary loops •Mesangial proliferation and matrix expansion and basement membrane thickening •Renal allograft biopsy with C4d deposition (in brown) in peritubular capillaries consistent with antibody- mediated rejection Fletcher J, et al. Pediatr Nephrol 2009
Management strategies in CAD Preventive -Careful selection of donor and recipient - Prevention and treatment of acute rejection - Prompt treatment of SCR by protocol biopsy - Identification and treatment of CMV/BK virus Therapeutic -Changes in currentimmunosuppressive protocols may increaselong-term renal allograft survival and function by decreasing both the risk of CAN and the risk of CVD -Selection of immunosuppressive regimen to halt or reverse CAN centered on avoidance or minimization of CNI - Preferred regimen: MMF+ Steroid± mTOR inhibitor/balatacept
With the introduction of induction therapy and more potent immunosuppressants the incidence of acute rejection has decreased significantly and SCR is almost unlikely which obviate the need for protocol biopsy • However the chance of BKV infection has increased several folds which causes CAD if not properly addressed
Merits of mTOR inhibitors over other immunosuppressants in selected patients • mTOR inhibitor causes: • Prolongation of graft survival -Prevention of CAN -Avoiding CNI nephrotoxicity • Decreased incidence of Coronary Artery disease • Decreased incidence of malignancy * Therefore with the use of mTOR inhibitors one can improve both graft as well as patients survival
Treatment of acute AMR • Plasmapheresis • Intravenous immunoglobulin • Modification of immunosuppressive regimen • Rituximab to reduce further antibody production by inhibiting B cells
Protocol Biopsies • Processes that lead to late graft loss begin early as SCR and can be detected by protocol biopsies (1,2,3,6 &12 M) • Chronic tubulo-interstitial and vascular changes can be seen in one third of transplants after 1 year and at later times become nearly universal • Detection of abnormalities in early protocol biopsies (the presence of IF/TA) is predictive of subsequent graft function and loss • Biopsies at 3 months scored as Banff ci0 have a significantly better graft survival at 5 years • Early treatment may have a dramatic effect on the outcome of the graft
Treatment of Sub-clinical Rejection • 72 patients: randomized to biopsies at 1, 2, 3, 6, and 12 months •SCR: treated during the first 3 months with methylprednisolone boluses • Treatment of SCR was associated with a reduced progression of IF/TA at 6 months and better graft function at 10 years , Rush D, et al. J Am Soc Nephrol 1998
BK Nephropathy • The prevalence rate varies from 1% to 10% depending upon the type of immunosuppressive protocols and diagnostic approaches • Pathophysiology: • Replicates best in uroepithelial cells, but also found in lymphoid, other tissues • Asymptomatic viruria → viremia • Ureteral ulceration, stricture & stenosis, hemorrhagic cystitis • Progressive loss of renal allograft function • Urothelial malignancy & vasculopathy
Screening and Diagnostic Testing for BK • Blood and/or urine samples every 3 months for first 2 years, then once a year and in the event of allograft dysfunction • Careful reduction of immunosuppression and close follow-up for development of acute rejection
BK Nephropathy •Intranuclear inclusion bodies in epithelial cells and severe tubular injury •Interstitial fibrosis •Positive immunohistochemical staining •Electron microscopy demonstrating viral particles
Impact of Reduction of Immunosuppression • Management of immunosuppression: • Identification of BK viremia triggered discontinuation of AZA or MMF • If viremia failed to clear within 4 weeks, the calcineurin inhibitor dose was tapered to trough CsA levels of 100– 200 ng/mL or trough TAC levels of 3–5 ng/mL • After reduction of immunosuppression, viremia resolved in 95%, without increased acute rejection, allograft dysfunction or graft loss • No BK nephropathy was observed on long-term follow up Brennan DC, et al. Am J Transplant 2005
Treatment of BK Nephropathy • No specific antiviral drug treatment • Reduction/adjustment in immunosuppression remains the cornerstone • Cidofovir, leflunomide, quinolones, and intravenous immunoglobulin: no randomized prospective clinical trial
Hypertension after Kidney Transplantation • Very common • Not well controlled-despite multiple antihypertensive medications • Independent risk factor for graft failure and mortality •ACE inhibitor/ARB preferred • Calcium blockers,β blocker,alpha blocker Kasiske B, et al. Am J Kidney Diseases 2004 Opelz G, et al. Kidney International 1998
•The use of ACEI/ARB therapy was associated with longer patient and graft survival after renal transplantation (2,031 patients, transplanted 1990-2003) Heinze G, et al. J Am Soc Nephrol 2006
Risk of long-term graft loss • 1505 patients with biopsy-proven GN from Australia (1988-1997) • Most frequent causes of allograft loss at 10 years: 1. CAN, 2. Death with a functioning graft, 3. Recurrence • The incidence of allograft loss due to recurrence at 10 years was 8.4% and increased overtime • Recurrence is more frequent than acute rejection as a cause of allograft loss during first 10 years after transplant Briganti EM, et al NEJM 2002
Recurrent Glomerular Diseases (GN) • Recurrence of primary GN: FSGS, MPGN, IgA nephropathy • Recurrence of secondary GN: SLE, Henoch-Schönlein, HUS/TTP, anti-GBM disease • Recurrence of metabolic or systemic disease: diabetic nephropathy, amyloidosis, scleroderma, oxalosis, Fabry disease
Minimizing the Impact of CNI- induced Nephrotoxicity • CNI avoidance: not very successful in the past • Conversion: CNI withdrawal at 3-mo or 6-mo; conversion to mTOR inhibitor • Minimization of CNIs + additional agents: low dose CNI with MMF + mTOR inhibitors ± steroids
Evaluation of a Patient with Late Allograft Dysfunction • Exclusion of obvious causes such as obstruction, dehydration, immunosuppression levels, uncontrolled hypertension, UTI etc • Urinalysis, spot urine ACR, 24h urinary protein • Doppler USG of the grafted kidney • BK viral load (blood/urine) •Kidney biopsy: consider early before significant graft dysfunction to differentiate between CNI toxicity,immune mediated changes or recurrent disease
Therapy for Chronic Allograft Dysfunction • Minimization of cold ischemia time • Aggressive management of hypertension: BP goal <130/80 mmHg • Management of diabetes/PTDM • Treatment of hyperlipidemia-LDL target<100 • Reduction of proteinuria • Treatment of infections-CMV/BK • Treatment of recurrent diseases
Therapy for Chronic Allograft Dysfunction • Manipulation of immunosuppression • More potent immunosuppressive therapy early after transplantation followed by minimization of immunosuppression, especially CNIs, to avoid CNI toxicity • Treatment of subclinical rejection • Monitoring and removal of HLA antibodies • Minimization or elimination of calcineurin inhibitors • Use of non-nephrotoxic immunosuppressive agents such as mTOR inhibitors/balatacept
Can we further improve the standard of care for our renal transplant patients? • To establish a reference Laboratory in the country for relevant immunological tests and drug level • To establish histopathology lab with dedicated renal histopathologist