Download

1 / 36
360 likes | 514 Vues
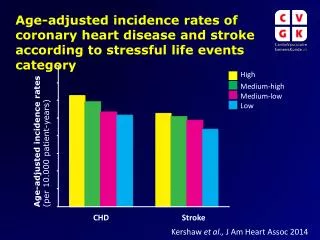
Developing Cost Effective CHD Screening Strategies. Leslee J. Shaw, PhD Department of Imaging and Medicine Cedars-Sinai Medical Center Los Angeles, California. CHD Detection In Asymptomatic Women & Men. Traditional approach to detection of CHD risk = assessment of typical risk factors

E N D
Developing Cost Effective CHD Screening Strategies Leslee J. Shaw, PhD Department of Imaging and Medicine Cedars-Sinai Medical Center Los Angeles, California
CHD Detection In Asymptomatic Women & Men • Traditional approach to detection of CHD risk = assessment of typical risk factors • Despite many available risk assessment approaches, there’s a detection gapfor asymptomatic individuals w/ subclinical atherosclerosis. • Framingham & European risk scores - useful “guides.” • to predict long term risk of CHD events in healthy populations. • Target Population for Screening: • 40% of the US Adult Population (or 36 million) = Intermediate Risk • Majority of 1st MIs Source: Abrams, Pasternak, Greenland, Houston-Miller, Smaha. BC #34: Taskforce #1 - Identification of CHD and CHD Risk. JACC 2003., Blumenthal, Becker, Yanek, Aversano, Moy, Kral, Becker. Detecting occult coronary disease in a high-risk asymptomatic population. Circulation 2003;107(5):702-707., Wilson, D’Agostino, Levy, Belanger, Silbershatz, Kannel. Prediction of CHD using risk factor categories. Circulation 1998;97:1837-1847.
X Source: Fletcher et al., 33rd Bethesda Conf: Preventive Cardiology: How Can We Do Better? JACC 2002;40:4:579-651., Wilson et al. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation 2001;103:1529-34., Jaffer et al. Age and Sex Distribution of Subclinical Aortic Atherosclerosis - A Magnetic Resonance Imaging Examination of the Framingham Heart Study Art, Thromb, Vasc Biol 2002;22:849.
Estimated 10 Yr. Hard CHD Risk Framingham Offspring & Cohort Women and Men Percent Women Men Age (years) Source: Abrams, Pasternak, Greenland, Houston-Miller, Smaha. Bethesda Conference #34: Identification of CHD and CHD risk: Is there a detection gap? JACC 2003
% Not Qualifying For Pharmacotherapy by CACS Women as well as young individuals were less likely to be considered candidates for pharmacotherapy vs. men & older individuals. Shaw Atherosclerosis (in press) - 45% low risk reclassified based on CAC Source: Nasir K, Michos ED, Blumenthal RS, Raggi P. Detection of High-Risk Young Adults and Women by Coronary Calcium and National Cholesterol Education Panel-III Guidelines. JACC 2005 (in press).
Estimated Direct & Indirect Costs of Cardiovascular Diseases & Stroke United States: 2005 Source: Heart Disease and Stroke Statistics – 2005 Update.
Current State of Health Care System • ~50% of health care costs are for end-stage or hospital care. • Avg yrly health expenditure for end stage care is ~5-x higher vs. non-end stage care. • Shifting care to early, diagnostic or outpatient sector potential to reduce cost. $412 Billion Medicare pays 31% $286 Billion Medicare pays 21% $122 Billion Medicare pays 2% $92 Billion Medicare pays 10% $60 Billion Medicare pays 0% $39 Billion Medicare pays 12% $37 Billion Medicare pays 0% $32 Billion Medicare pays 29% $31 Billion Medicare pays 4% $19 Billion Medicare pays 25% Source: CMS, Office of the Actuary, National Health Statistics Group. Access date: March 2, 2004.
Medicare Spending - 2/3rds of Spending = 5+ Chronic Conditions - 1/5th of Spending = 3+ Chronic Conditions Source: Medicare Standard Analytic File, 1999.
The Most Expensive Conditions In America: MEPS Population Estimates BillionBillion 1. Ischemic Heart Disease $21.5 9. Cerebrovascular Dz $8.3 2. Motor Vehicle Accidents $21.3 10. Dysrythmias $7.2 3. Acute Resp. Infections $17.9 11. Peripheral Vascular $6.8 4. Arthropathies $15.9 12. COPD $6.4 5. Hypertension $14.8 13. Asthma $5.7 6. Back Problems $12.2 14. CHF $5.2 7. Mood Disorders $10.2 15. Lung Cancer $5.0 8. Diabetes $10.1
The Most Expensive Conditions In America: MEPS Population Estimates BillionBillion 1. Ischemic Heart Disease $21.5 9. Cerebrovascular Dz $8.3 2. Motor Vehicle Accidents $21.3 10. Dysrythmias $7.2 3. Acute Resp. Infections $17.9 11. Peripheral Vascular $6.8 4. Arthropathies $15.9 12. COPD $6.4 5. Hypertension $14.8 13. Asthma $5.7 6. Back Problems $12.2 14. CHF $5.2 7. Mood Disorders $10.2 15. Lung Cancer $5.0 8. Diabetes $10.1
Upfront Test Cost Affected by MD Labor, Lab Volume, +/- Add-Ons (Contrast or Radiopharmaceutical), Equipment (Lease, Age, Shared) Low Cost Lab / Office Visit Cardiac Imaging Source: Mark DB, Shaw LJ, et al. Bethesda Conference #34- Taskforce #5 - Is atherosclerotic imaging cost effective? JACC 2003;41:1906.
Average Cost Inputs for Adverse Sequelae of CVD • Out-of-Hospital SCD – Lost Productivity • In-Hospital Death – in excess of $50k-$100k • End-Stage Care for CHF – 80% of lifetime care costs • AMI or ACS $15-20k • Chest Pain Hospitalization $6k • Stroke $50k • Anti-Ischemic Rx $1,500 - $5,000 / yr • Out-of-Pocket $2,000 / yr • ….
Medicare Payment Advisory Commission (MedPAC) - Growth in Physician Services Growth of All Physician Services % 22% Includes all Services in the Physician Fee Schedule Source: MEDPAC Analysis of Medicare Claims Data March 17, 2005, Executive Director, Medicare Payment Advisory Commission, Mark Miller,.htm
Trends in CV Operations & Procedures United States: 1979-2000
Unfolding a Body of Evidence Building Building • Observational • Data • Risk identification • Costs • Cost Effectiveness • High Risk CEA • Reimbursement • Clinical Trial • Data • Vs. Comparators • Disease Management • Risk Identification • Cost Efficiency • Outcomes – Improve Process of Care • Quality Standards: • Benchmarking / Profiling • Cost / Charges • Guiding Providers • Adherence Guidelines Practice Guidelines / Critical Pathways Source: Shaw LJ, Redberg RF. From clinical trials to public health policy: The path from imaging to screening. Am J Cardiol 2001 Jul 19;88(2-A):62E 65E.
Basics of CEA • CEA – technique for selecting among competing choices when resources are limited. • “Value for Money” • Technique comparing relative value of various clinical strategies. Commonly, a new strategy is compared w/ current practice (i.e., "low-cost alternative") in calculation of CE ratio: • Result = "price" of an additional outcome purchased by switching from current practice to new strategy (e.g., $10,000 / life year). If the price is low enough, new strategy is considered "cost-effective.“ • =Standard: <$50,000 / LYS Source: http://www.acponline.org/journals/ecp/sepoct00/primer.htm
Critical Cost Effectiveness (CE) Questions • 1. Vs. usual care—i.e., no screening—what is the CE of CHD screening of asymptomatic adults to reduce risk for CHD-specific morbidity / mortality? • 2. What is the CE of selective screening adults at increased risk for CHD — e.g., those with a family history of premature CHD, w/ risk factors — vs. routine screening & usual care? • 3. How will differences in rx effectiveness affect CE estimates for CHD screening? • 4. Among individuals w/ subclinical disease on initial screening exam, what is the CE of periodic surveillance vs. one-time screening? • 5. Among individuals w/out subclinical CAD on initial screening exam, what is the CE of re-screening at varying intervals vs. onetime screening?
Screening Criteria Discussed • Burden • Prevalence of disease • Years of life lost • Disability or quality of life • Economic burden • Effectiveness and Efficacy • Cost effectiveness • Current delivery rates • Feasibility of increasing delivery rates
Cost Effective CHD Screening • 1. Detection of Risk • 2. Early Rx • 3. Improved Outcome • Resulting in Reduction in More Costly, End-Stage Care • Improved Societal Productivity
Evaluation Criteria • Burden of disease • Single measure incorporating mortality & morbidity • Effectiveness of Screening • Cost effectiveness • Feasibility of Increasing Delivery Rates
CHD Screening Framework Two Steps: • Burden and Effectiveness into single measure of Clinically Preventable Burden (CPB) • Cost Effectiveness included to account for resource consumption
Clinically Preventable Burden • CPB = Burden x Effectiveness • Burden includes all disease targeted by CHD • Effectiveness = % of burden reduced • Measures burden of CHD preventable • Burden measured in Quality-Adjusted Life Years Saved (QALYS) -- approximated • Uses effectiveness from RCT • Range of Therapeutic Risk Reduction
Clinically Preventable Burden • Qualitative assessment of CHD screening should consider: • CPB - not burden and effectiveness separately • focus on fatal or high-prevalence, nonfatal conditions • Costs of service: medical care, out-of-pocket • Potential for cost savings
Cost Effectiveness (CE) Analysis • CE = costs of screening – costs averted Net Effectiveness** • ICER = • CHD Screening vs. No Testing / Usual Care • CHD Screening vs. Global Risk Score • CHD Screening vs. Alternative Testing • CAC vs. C-IMT • CAC vs. BART • CAC vs. …. • ** Clinically Preventable Burden reduced
Treatment-Eligible US-Population under NCEP II, NCEP III, CAC Screening Men Women NCEP II NCEP III CAC Millions of people Age (y) % Increase 142.5 184.3 124.9 85.9 65.0 50.0 65.0 50.0 Source: Fedder DO et al., Circulation 2002;105:152-156, Nasir K, Michos ED, Blumenthal RS, Raggi P. Detection of High-Risk Young Adults and Women by Coronary Calcium and National Cholesterol Education Panel-III Guidelines. JACC 2005 (in press).
Treatment Est. 10-Yr Costs from NCEP III to CAC Screening Men Women NCEP III CAC Millions of $ Source: Fedder DO et al., Circulation 2002;105:152-156, Nasir K, Michos ED, Blumenthal RS, Raggi P. Detection of High-Risk Young Adults and Women by Coronary Calcium and National Cholesterol Education Panel-III Guidelines. JACC 2005 (in press).
Relative Risk (RR) Ratios (95% CI) by CACS Risk Events / N CACS RR (95% CI) p Value 0.01 0.1 1 10 100 Summary RR Ratio Higher Risk Low Risk Very Low Risk 1-44 1.5 (0.8-2.9) 24 / 6931 18 / 8503 0.18 Low Risk 1-112 2.1 (1.3-3.3) 46 / 2670 26 / 4600 0.003 Moderate Risk 100-400 4.1 (2.9-6.0) 102 / 4,428 44 / 9,977 <0.0001 High Risk 400-999 6.7 (4.8-9.4) 179 / 3,550 44 / 6,839 <0.0001 Very High Risk* 1,000 10.8 (4.2-27.7) 14 / 196 6 / 905 <0.0001 0.01 0.1 1 10 100 Lower Risk Higher Risk Very Low Risk includes Kondos, LaMonte, Taylor When c/w FRS event rates, Δ LYS with CACS 0.58 for 35% RR Reduction w/ Rx (0-0.83) Low Risk includes Arad, Greenland, LaMonte Moderate Risk includes Arad, Greenland, LaMonte, Taylor, Vliegenthart High Risk includes Arad, Greenland, Kondos, LaMonte, Vliegenthart Very High Risk includes Vliegenthart
CPB Model Inputs – Disease Burden Source: MI rates were extrapolated from ARIC, 1987-2000 & does not include silent MIs. CVA data also not included.
CPB Model Inputs – Disease Burden Source: MI rates were extrapolated from ARIC, 1987-2000 & does not include silent MIs. CVA data also not included.
CPB Model Inputs – Procedure Burden Source: CDC/NCHS for 2002. http://www.acc.org/advocacy/word_files/2005ProposedPhysicianPmtRulev3%20web.xls.
CPB Model Inputs – Procedure Burden Source: CDC/NCHS for 2002. http://www.acc.org/advocacy/word_files/2005ProposedPhysicianPmtRulev3%20web.xls.
Markov Model:Health states - ovals; arrows represent allowed transitions. All pts start event-free & can remain, have MI or angina, or die. Event-Free Post-MI Post-AP Death Post-MI & AP Markov model to estimate the benefits, costs, & incremental cost-effectiveness of CHD screening followed by targeted statin rx for high risk subclinical dz, vs. usual care alone, for the primary prevention of CV events among patients ages 45-65 years.. Source: Blake GJ, Ridker PM, Kuntz KM. Potential Cost-effectiveness of C-Reactive Protein Screening Followed by Targeted Statin Therapy for the Primary Prevention of Cardiovascular Disease among Patients without Overt Hyperlipidemia. Am J Med 2003;114:485– 494.
Multi-Attribute Cost Markov Model:Comparing FRS vs. CACS for 5 Yrs. Of Observational Follow-up Estimated LYS in Pts. Ages 45-65 yrs. Event-Free Event-Free FRS CACS Death Death Post-MI & AP Post-MI & AP <$50,000 / Events Averted
Conclusions • If we can identify w/ a high degree of likelihood pts at risk for AMI / SCD, then it is likely that a CV screening-driven approach including prevention (i.e., risk factor modification) can result in improved outcomes & aversion of costly hospitalizations. • Preliminary analyses from the CE models reveal that subclinical dz screening can be cost effective when applied to “higher risk” or appropriate patient candidates. • When compared with global risk scores that often underestimate risk in key patient subsets: women, young, international cohorts. • Decision models do not replace RCT comparing an array of imaging modalities, laboratory markers, or global risk scoring.
Potential Evidence for Priority Setting • Priority Criteria Measures • Impact • Condition Disability, Mortality • System Costs, Guideline Adherence, Errors • Societal Indirect Costs • Improvability • Condition Cost-Effectiveness, efficacy • Disparity Impact on vulnerable subgroups • System Effectiveness of quality improvement • Inclusiveness Diffusion across subpopulations
Unmet Expectations & Limitations to CHD Screening • Many preventive services are recommended • Delivery of effective services is incomplete • Resources—time and money—are limited • Preventive services differ in their health impact and costs