Download
1 / 31
310 likes | 519 Vues
The Hospital Market, Part 2. Professor Vivian Ho Health Economics Fall 2007. Structure: Putting it all Together. Is the hospital market competitive, or not? Case Study : UNITED STATES OF AMERICA, Plaintiff, vs. MERCY HEALTH SERVICES and FINLEY TRI-STATES HEALTH GROUP, INC. Defendants.

E N D
The Hospital Market, Part 2 Professor Vivian Ho Health Economics Fall 2007
Structure: Putting it all Together Is the hospital market competitive, or not? Case Study: UNITED STATES OF AMERICA, Plaintiff, vs. MERCY HEALTH SERVICES and FINLEY TRI-STATES HEALTH GROUP, INC. Defendants.
Filed October 17, 1995 • Mercy and Finley: only 2 acute care hospitals in Dubuque, Iowa propose to merge. • Justice Department sues for preliminary injunction.
Facts Dubuque population = 86,403 Mercy: 320 staffed beds, average daily census = 127. Finley: 124 staffed beds, average daily census = 63.
competition - outside 70m radius, but within 100 m. Madison, Wisconsin Waterloo Cedar Rapids Dubuque Freeport, Illinois Iowa City, Iowa
Insurance coverage for Mercy/Finley patients • 50% Medicare/Medicaid • 25% Fee-for-service (traditional indemnity) • 25% Managed care (HMOs, PPOs) • Negotiated 15-30% hospital price discounts.
Justice Department case 1) Where do Dubuque patients go for hospital care? 88% inside (Mercy or Finley) 12% outside 2) Where are Mercy/Finley patients from? 76% inside (Dubuque) 24% outside • Dubuque the relevant geographic market, and merger constitutes a monopoly.
Ruling • District court judge rejects Justice Department’s definition of geographic market as too narrow. • “The government continues to fail to look at the merger within the context of current market trends. All evidence is that there is a great deal of competition for health care dollars…”
“…if DRHS [merged entity] reacted in a noncompetitive manner, an HMO that could successfully induce Dubuque area residents to use alternative hospitals would be at a significant cost advantage.” • “There is also evidence that managed care entities can successfully induce Dubuque residents to use other regional hospitals for their inpatient needs.” Merger of Mercy and Finley would not/could not result in higher prices.
Case Study Conclusion • Even if only one hospital exists in a given geographic region, it may not be able to act as a monopolist • Ability of large, managed care buyers to shift patients can keep the market competitive.
Hospital Advertising • % of hospitals that advertise rose from 36% in 1995 to 50% in 1998. • We often see ads for local hospitals in newspapers and magazines. • Why?
Dorfman-Steiner model of advertising • The profit-maximizing amount of advertising occurs where: • If Ea equals .2, then 1% ↑ in advertising → .2% ↑ in demand. • And if EP equals 4, then Ea / EP 0.05 • To max profits, hospital should spend 5% of total revenues on advertising.
Hospital will spend more on advertising when: • Ea is higher. • EP is lower. • ↑ advertising costs $. But when demand is less elastic with respect to price, these costs can be passed onto the consumer. • Hospitals with greater market power will advertise more aggressively.
What type of advertising will hospitals use? • Advertising the availability of services that all hospitals have may ↑market size, but not your own patient base. • Hospitals will use advertising to differentiate their product. • Hospital rankings. • Luxury services.
Hospital Conduct • Large #s of sellers and low barriers to entry promote competition. • We expect increased competition to lead to: • Higher output and quality. • Lower price.
However, the hospital market has important differences. • Hospitals don’t necessarily maximize profits. • Government is a major payer • Prices not set competitively. • Consumer less likely to shop around. • Insurance and asymmetric info. • Is hospital market competition good or bad for consumers?
Markets with fewer hospitals may face higher prices. • But hospitals in more concentrated markets may be larger, and econ of scale may ¯ costs. • Look at price and quality effects of hospital mergers.
Data from Los Angeles in 1990-1993 suggests that hospital mergers would ↑ prices >5%. • (Town & Vistnes 2001) • Hospitals that merged between 1989 and 1996 lowered their costs two years after consolidation relative to comparable hospitals that didn’t merge • (Dranove & Lindrooth 2003) • Even if hospitals lower costs, they may not pass price savings on to consumers. • Hospitals that merged in 1997-2001 raised their negotiated PPO prices relative to the median market price.
Other studies suggest that hospital consolidation does not improve the quality of care. • These results suggest that more competitive hospital markets favor consumers.
Does Ownership Type Affect Conduct? • Empirical Evidence • Prices higher for for-profit hospitals, but NFP & public hospitals enjoy tax advantages, municipal bond discounts. • Only small differences in costs by ownership type.
But public hospitals provide more uncompensated care • Data from CA calls into question tax-exempt status of NFPs.
Has managed care changed conduct? • Empirical Evidence • HMO hospitalization rates 15-20% lower than those of fee-for-service insurance plans. • However, HMO growth has not led to decrease in total hospital costs per capita at market level.
Maybe further HMO penetration required. • Government still a dominant payer, and reimburses generously. • Maybe managed care doesn’t work. • Outcomes for patients covered by HMOs similar & sometimes better than those for fee-for-service patients.
Hospital Market Performance How have price and quantity changed?
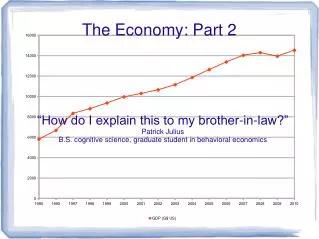
Source: U.S. Department of Labor, Bureau of Labor Statistics, CPI Detailed Report (various issues).
Hospital inflation rate exceeds general rate for all but 1 year. • Despite move to prospective reimbursement by Medicare in 1983, hospital inflation continued. • Possible explanations 1) generous insurance 2) fee-for-service medicine 3) lack of profit motive 4) quality competition
What about Quantity? • . Average length of stay declined, and admissions and occupancy rates declined through the 1990’s. • 2. But staffing, outpatient visits rose. Source: American Hospital Association, Hospital Statistics
Was growth in staffing, outpatient visits inappropriate? Ratings of inappropriate use of 3 medical treatments among 1981 Medicare population, as defined by expert panel of MDs. Procedure Inappropriate use(%) coronary angiography 17% carotid endarterectomy 32% upper GI tract endoscopy 17%
Similar findings in 1979-1982 for coronary artery bypass graft patients. • More recent studies find less inappropriate use in New York. • However, practice variation studies show many surgical procedures performed less often relative to other areas in U.S.
Source: Marc L. Berk and Alan C. Monheit, “The Concentration of Health Expenditures: An Update,” Health Affairs 20 (Spring 2001), Exhibit 1.
Distribution of health expenditures has become more concentrated. • Most severely ill patients receiving high-cost critical care in hospitals. • 1/7 of all health expenditures spent on those in last 6 months of life. • Do we need to ration health care costs for the very ill?