Download
1 / 59
2.09k likes | 8.1k Vues
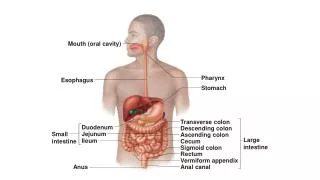
Disorders of oral cavity. dr shabeel pn. Actinic cheilitis Premalignant condition due to chronic UVR exposure Affects lower lip, initially edematous & erythematous, later atrophic, white, scaly plaque, may obliterate vermillion border

E N D
Disorders of oral cavity dr shabeel pn
Actinic cheilitis Premalignant condition due to chronic UVR exposure Affects lower lip, initially edematous & erythematous, later atrophic, white, scaly plaque, may obliterate vermillion border Ulceration or induration - biopsy to rule out malignant transformation Disorders of the Lips
Angular cheilitis (perleche) Inflammatory reaction- erythema and maceration at the angles of mouth, fissuring and crusting may be present Predisposing factors- advanced age, ill-fitting dentures, thumb-sucking in children, oral Candidiasis, bacterial infections Disorders of the Lips…
Disorders of the Lips… • Cheilitis glandularis • Inflammatory painless enlargement of lower lip, usually in elderly men • Triggered by actinic damage, bacterial infection, tobacco exposure, chronic irritation • Chelitis glandularis apostematosa • Painful enlargement, eversion of lip with erosions and recurrent bacterial infections or malignant transformation
Exfoliative cheilitis (factitious cheilitis) Chronic superficial inflammation of vermilion borders of the lips Characterized by persistent scaling Attributed to repeated lip sucking, chewing or other manipulation of lips Disorders of the Lips…
Granulomatous inflammation, acute onset of asymmetric swelling of the upper lip or lower lip Erythema, scaling, fissuring and erosions may develop Prolonged and recurrent course with eventual fixed swelling May be associated with constitutional symptoms, regional lymph node enlargement Granulomatous cheilitis (cheilitis granulomatosa)
Granulomatous cheilitis • Melkersson-rosenthal syndrome- triad of lingua plicata ( fissured or furrowed tongue), facial paralysis and granulomatous cheilitis • Other cranial nerves (olfactory, auditory, glossopharyngeal, hypoglossal) may be involved • Biopsy- oedema, perivascular lymphocytic infiltrate, focal granulomas resembling sarcoidosis or Crohn’s disease
Disorders of Tongue • Glossodynia (burning mouth syndrome)- spontaneous burning, discomfort, pain, irritation, or rawness of the tongue, has no identifiable etiology most of the time • Etiology- • Idiopathic, Infection, Allergic/contact hypersensitivity, Mechanical trauma • Xerostomia, Geographic tongue/ Fissured tongue • Vesiculobullous disease, temporomandibular dysfunction • Referred pain from teeth or tonsils • Drugs- Antibiotics, psychiatric medications, chemotherapy
Neurologic Peripheral nerve damage Diabetic neuropathy Trigeminal neuralgia Acoustic neuroma psychiatric Depression Anxiety Cancerophobia Somatoform disorder OCD Systemic disorders Anemia (iron deficiency, pernicious) Nutritional deficiency Gastroesophageal reflux disease Sjogren syndrome Hypothyroidism Acquired immunodeficiency syndrome Etiology of Glossodynia
Disorders of Tongue… • Glossitis- presents as pain, irritation or burning, hypogeusia, or dysgeusia • Atrophic glossitis • Due to filiform de-papillation • Mild patchy erythema to a completely smooth, atrophic, beefy-red surface • Etiology - pernicious anemia, protein and other nutritional deficiencies, chemical irritants, drug reactions, amyloidosis, sarcoidosis, vesiculobullous diseases, oral candidiasis and systemic infections • Moeller or Hunter glossitis of pernicious anemia affects the lateral aspects and tip of the tongue respectively
Median rhomboid glossitis - atrophic disorder of the tongue secondary to chronic candidiasis Disorders of Tongue…
Geographic tongue- benign inflammatory condition, due to Loss of filiform papillae Erythematous plaques with an annular or serpiginous well demarcated white border Etiology- psoriasis, Reiter syndrome, atopic dermatitis, diabetes mellitus, anemia, hormonal disturbances, Down syndrome, lithium therapy Disorders of Tongue…
Fissured tongue (furrowed tongue, scrotal tongue, grooved tongue) normal variant seen in 5-11% individuals Numerous small irregular fissures oriented laterally on the dorsal tongue Also seen in - Melkersson-Rosenthal syndrome, psoriasis, Down syndrome, acromegaly, Sjogren syndrome Disorders of Tongue…
Herpetic geometric glossitis - rare cause of fissuring of tongue, presents with acute onset of pain and deep longitudinal grooves with smaller lateral fissures Disorders of Tongue…
Hairy tongue (white or black hairy tongue) - hypertrophy of filiform papillae resembling hair-like projections Associated with - heavy tobacco use, mouth breathing, antibiotic therapy, poor oral hygiene, general debilitation, radiation therapy, chronic use of bismuth containing antacids, lack of dietary roughage White, yellow green, brown, or black color is due to chromogenic bacteria or staining from exogenous sources Disorders of Tongue…
Orai hairy leukoplakia- caused by Epstein-Barr virus, presents as asymptomatic, corrugated, white plaques with accentuation of vertical folds along the lateral borders of tongue Predominantly seen in HIV infection, organ transplant recipients and patients on chemotherapy Disorders of Tongue…
Disorders of Tongue… • Macroglossia- congenital or acquired process, tongue is disproportionately large relative to the patient’s jaw size • Difficulty with mastication and speech and accidental tongue biting are common • Differential- Down syndrome, hypothyroidism, Beckwith-Wiedemann syndrome, neurofibromatosis, infection by mycobacteria, filamentous bacteria or fungus, amyloidosis
Disorders of Salivary Glands • Xerostomia (dry mouth) - decreased saliva production • Women are twice as affected as men • Signs and symptoms - diminished or altered taste and smell, halitosis, heavy plaque accumulation, difficulty in wearing dentures, recurrent yeast infections, burning sensation, difficulty swallowing, dry or cracked lips, salivary calculi and increased thirst
Causes of xerostomia • Medications - Antidepressants, antihistamines, diuretics • Medical conditions - Parkinson disease, diabetes, anemia, cysticfibrosis, rheumatoid arthritis • granulomatous inflammation - tuberculosis, sarcoid, Sjögren syndrome, HIV, amyloid • Dehydration - Fever, excessive sweating, vomiting, diarrhea, blood loss, burns, smoking, consumption of tea, coffee • Radiation therapy of head and neck • Surgical removal of the salivary glands • Old Age
Mucocele (mucous retention cysts)- benign, painless, dome- shaped fluctuant papules, due to trauma or obstruction of minor salivary gland ducts Multiple mucoceles - graft vs host disease, lichen planus, cicatricial pemphigoid Ranula - large, bluish, translucent fluctuant mass in the floor of the mouth due to obstruction of the submandibular and or sublingual duct Diffuse parotid gland enlargement - acute mononucleosis, HIV infection Disorders of Salivary Glands
Disorders of Gingiva & Periodontium • Gingivitis - erythema, edema, and blunting of the interdental papillae, without bone loss • Predisposing factors - poor oral hygiene, tobacco use, diabetes • Periodontitis -chronic infection of connective tissue, periodontal ligament and alveolar bone • Long-term penodontitis is associated with increased risk of diabetes, heart disease, stroke and preterm birth • birth control pills, diabetes, steroids, Down syndrome, Langerhans cell histiocytosis, HIV predispose to periodontitis • Juvenile periodontitis is associated with genetic defects in leukocyte chemotaxis • Papillon-Lefevre syndrome - severe and destructive periodontal disease, with exfoliation of the deciduous and permanent teeth
Disorders of Gingiva & Periodontium • Erosive gingivostomatitis (desquamative gingivitis)- inflammation and erythema of the gingiva, nonspecific reaction pattern, may be due to viral infection, autoimmune, inflammatory and blistering disorders • Lichen planus - painful or asymptomatic lacy white patches, plaques or papules, often with erosions and ulcerations • Lichenoid mucositis - NSAIDS, antihypertensive medications, contact allergy, graft-versus-host disease
Acute necrotizing ulcerative gingivitis (trench mouth, vincent disease) Punched- out ulcers of the interdental papillae, gingival hemorrhage, severe pain, foul odor Fever and lymphadenopathy are common Precipitating factors- poor oral hygiene, nutritional deficiency, alcohol and tobacco use, Immunosuppression Etiologic agents- Treponema, Selenomonas, Bacteroides, Prevotella and Borrelia vincentii Disorders of Gingiva & Periodontium
Aphthous ulceration • Acute, recurrent, painful ulcers on nonkeratinized mucosa • Most common cause of oral ulcerations • Effect up to 30 % of the population • Ulcers with a gray or yellow pseudomembrane and erythematous margin • Potential triggers - heredity, food and medication allergy, decreased mucosal barrier integrity, hematologic and immunologic disorders, emotional stress, and trauma
Aphthous ulceration • Systemic Conditions Associated • Hematinic deficiency (up to 20%)- iron, folic acid or vitamin B12 deficiency • Gastrointestinal malabsorption (3%) - Celiac disease, dermatitis herpetiformis, gluten-sensitive enteropathy, Crohn disease, pernicious anemia • Systemic lupus erythematosus, reactive arthritis • HIV • Behcet disease • PFAPA (periodic fever, aphthous stomatitis, pharyngitis, and cervical adenitis) • MAGIC (mouth and genital ulcers with inflamed cartilage)
Major criteria Oral Aphthae Genital Ulcers Ocular- Iridocyclitis, Retinal vasculitis,Optic atrophy CNS lesions- Meningoencephalitis, cerebral infarction, psychosis, cranial nerve palsies, cerebellar and spinal cord lesions Dermatological Pustules Erythema nodosum Pathergy Minor criteria Proteinuria and haematuria Thrombophlebitis Aneurysms Arthralgias Behcet’s disease
Non-aphthous erosions & ulcers • Pemphigus vulgaris, paraneoplastic pemphigus, bullous pemphigoid, cicatricial pemphigoid, EB acquisita • Epidermolysis bullosa simplex, junctional EB & dystrophic EB demonstrate the most severe • Discoid and SLE- oral discoid lupus is characterized by “sunburst” erythematous plaques surrounded by white radiating striations • Erythema multiforme and stevens-johnson syndrome/toxic epidermonecrolysis
Non-aphthous erosions & ulcers… • Chronic ulcerative stomatitis - autoimmune mucosal erosive disorder • Resemble erosive LP • Direct immunofluorescence- IgG bound to nuclei of keratinocytes of basal and lower epithelial layers • Responsive to Hydroxychloroquine
Iatrogenic mucositis • Complications of systemic chemotherapy and head and neck radiation, occurs due to direct tissue injury of the mucosal epithelium
Localized Amalgam, tattoo Ephelis / Naevus Malignant melanoma Kaposi’s sarcoma Peutz–Jegher syndrome Laugier–Hunziker syndrome Melanotic macules Generalized Racial Localized irritation, e.g. smoking Drugs, e.g. phenothiazines, antimalarials, minocycline, contraceptives, mephenytoin Addison’s disease/ Nelson’s syndrome Ectopic adrenocorticotrophic hormone (e.g. bronchogenic carcinoma) Albright’s syndrome Haemochromatosis Neurofibromatosis, incontinentia pigmenti Malignant acanthosis nigricans Disorders of mucosal pigmentation
Benign Tumors • Pyogenic granuloma (pregnancy tumor) - an exaggerated, reactive proliferation of granulation and vascular tissue triggered by minor trauma or medication, classically during pregnancy • Pulp polyp- exaggerated reactive proliferation of the dental pulp (neurovascular bundle), results when gross caries destroys the enamel crown • Verruciform xanthoma - minute white or yellow verrucous papules on the gingiva, alveolar mucosa, or hard palate. Foamy, lipid-laden macrophages in biopsy • Mucosal lipomas - present as asymptomatic, soft, yellow nodules on the buccal or vestibular mucosa, tongue, floor of the mouth or lips of middle-aged adults
Benign Tumors… • Traumatic neuroma - occur around mental foramen, alveolar ridge, lip or tongue • Neurofibromas and schwannomas (neurilemmoma) - on the tongue or buccal mucosa • Sipple syndrome - multiple mucosal neuromas, associated with pheochromocytoma, parafollicular thyroid cysts secreting calcitonin, medullaiy thyroid carcinoma and opaque nerve fibers on the cornea • Granular cell tumor (Abrikosov tumor) - reactive process of Schwann cell origin, appears on the dorsal tongue as single or multiple asymptomatic firm, ill-defined papule
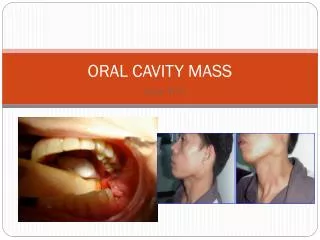
Pre-Malignant Lesions • Leukoplakia - chronic, white, verrucous plaque with histologic atypia • Severity linked to the duration and quantity of tobacco and alcohol use • Occur anywhere in the oral cavity • Lip, tongue, or floor of the mouth lesions are prone for progression to SCC • Erythroplakia - non-inflammatory erythematous plaque • Analagous to intra-oral erythroplasia of Queyrat or SCC in situ • Biopsies - severe dysplasia and areas of frank invasion
Pre-Malignant Lesions… • Submucous fibrosis • generalized white discoloration of oral mucosa with progressive fibrosis, painful mucosal atrophy and restrictive fibrotic bands • individuals who chew betel quid, a concoction of tobacco, lime, areca nut and betel leaves • Ultimately leads to trismus, dysphagia and severe xerostomia • 5 - 10 % progress to SCC
Malignant Lesions • Squamous cell carcinoma - present as leukoplakia, erythroplakia, erythroleukoplakia, irregular endophytic masses with ulceration or exophytic nodules • High-risk anatomic sites - ventrolateral tongue, floor of the mouth, and the vermillion border of the lip • Verrucous carcinoma - locally aggressive SCC in older adults presents as a hyperkeratotic, verrucous, exophytic white mass on the vestibules or mandibular gingiva, floor of the mouth, palate, and lip. Risk factors - smokeless tobacco and infections with HPV( 16 and 18)
Malignant Lesions… • Proliferative verrucous leukoplakia - rare progressive multifocal leukoplakia, with white, hyperkeratotic, verrucous plaques involve large areas of mucosa • Women are affected four times as men • More than 90 % undergo malignant transformation • Smoking is not associated, HPV may be etiologic factor • Melanoma - irregular pigmented macule, patch or papule on the hard palate or maxillary gingiva • in older than 50 years • advanced lesions may ulcerate or bleed • Breslow depth - most important prognostic factor
Malignant Lesions… • Hodgkin, non-Hodgkin, cutaneous Tcell, and Burkitt lymphoma - non-specific, indurated, painless masses • Burkitt lymphoma is associated with alveolar bone destruction • Langerhans cell histiocytosis - ulcerative gingivitis, periodontitis, ulceration and bony destruction, may be initial or sole manifestation of disease • multicentric reticulohistiocytosis - flesh-colored to reddish-brown nodules on oral or nasal mucosa, in addition to classic cutaneous lesions and associated arthropathy • Kaposi sarcoma - single or multiple hemorrhagic patches or exophytic nodules, most often on gingiva or palate
Varicosities • Asymptomatic, blue, soft nodules on the lips and ventrolateral tongue • Not associated with any known systemic disease • Caliber-persistent labial artery - raised pulsatile tortuous, blue rubbery bleb appreciation of lateral pulsation is diagnostic • Mucosal hemangiomas - benign vascular tumors of infancy, erythematous or bluish vascular nodules, sometimes with associated thromboses and phleboliths, spontaneous regression usual • Petechiae, ecchymoses, hematomas, and spontaneous gingival hemorrhage in thrombocytopenia, coagulation, hemolytic anemia, von willebrand disease, anticoagulant therapy
Salivary Gland Tumors • Occur most commonly on the palate and on the retromolar pad distal to the third molar • Erythematous papules or ulcerated papules and nodules
Physical and Chemical Trauma • Chronic biting and manipulation of lips in and buccal mucosa in nervous habit- ragged, irregular, white plaque at the site of trauma • Frictional keratosis - thickened white plaque (sharp tooth or overextended denture) • Irritation fibroma - sessile nodule at site of chronic mucosal irritation • Smoker’s palate or nicotine stomatitis - thermal injury to the hard palate of pipe smokers • Appears as a diffusely white palate studded with 2-5mm erythematous umbilicated papules
Physical and Chemical Trauma • Epulis fissuratum- • Develops beneath poorly fitting dentures, painless, elongated ridges of hypertrophic mucosa along the anterior labial alveolar ridge • Giant cell epulis • A reactive hyperplastic proliferation, appears as a deep red papule on the interdental papillae • Many multinucleated giant cells are seen histologically in a vascular proliferation
Chemical burn • Aspirin burns • Mucosa in direct contact with aspirin becomes necrotic and painful, also with Medications containing phenol • Contact stomatitis • Intra-oral erythema, ulceration or a lichenoid mucositis • Dental amalgams, Cinnamate, flavorings, food additives, spices, toothpaste, mouthwash, dental epoxy resins, cosmetic lip products