Download
1 / 57
610 likes | 1.01k Vues
25 Hepatitis Virus. Viral Hepatitis - Historical Perspective. Enterically transmitted. “ Infectious”. A. E. Viral hepatitis. NANB. Parenterally transmitted. B. D. C. “ Serum”. F, G, ? other. Viral Hepatitis - Overview. Type of Hepatitis. A. B. C. D. E. Source of. feces.

E N D
Viral Hepatitis - Historical Perspective Enterically transmitted “Infectious” A E Viral hepatitis NANB Parenterally transmitted B D C “Serum” F, G, ? other
Viral Hepatitis - Overview Type of Hepatitis A B C D E Source of feces blood/ blood/ feces blood/ virus blood-derived blood-derived blood-derived body fluids body fluids body fluids percutaneous Route of fecal-oral percutaneous fecal-oral percutaneous transmission permucosal permucosal permucosal Chronic no yes yes yes no infection Prevention pre/post- pre/post- blood donor pre/post- ensure safe exposure exposure screening; exposure drinking immunization immunization water risk behavior immunization; risk behavior modification modification
HEPATITIS A VIRUS • RNA Picornavirus • Single serotype worldwide • Acute disease and asymptomatic infection • No chronic infection • Protective antibodies develop in response to infection - confers lifelong immunity
Jaundice by <6 yrs <10% age group: 6-14 yrs 40%-50% >14 yrs 70%-80% • Rare complications: Fulminant hepatitis Cholestatic hepatitis Relapsing hepatitis • Incubation period: Average 30 days Range 15-50 days • Chronic sequelae: None HEPATITIS A - CLINICAL FEATURES
EVENTS IN HEPATITIS A VIRUS INFECTION Clinical illness Infection ALT IgM IgG Viremia Response HAV in stool 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Week
CONCENTRATION OF HEPATITIS A VIRUS IN VARIOUS BODY FLUIDS Feces Serum Body Fluids Saliva Urine 102 104 100 106 108 1010 Infectious Doses per mL
HEPATITIS A VIRUS TRANSMISSION • Close personal contact(e.g., household contact, sex contact, child day-care centers) • Contaminated food, water(e.g., infected food handlers) • Blood exposure (rare)(e.g., injection drug use, rarely by transfusion)
PREVENTING HEPATITIS A • Hygiene (e.g., hand washing) • Sanitation (e.g., clean water sources) • Hepatitis A vaccine (pre-exposure) attenuated virus or inactivated virus • Immune globulin (pre- and post-exposure)
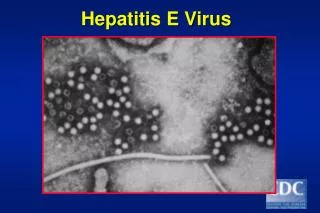
HEV is a 30-32nm non-enveloped particle containing a s/s (+)sense RNA genome of ~7.5Kb. • Genetic organization similar (not identical) to Caliciviruses:
Hepatitis E - Clinical Features • Incubation period: Average 40 days • Range 15-60 days • Case-fatality rate: Overall, 1%-3% Pregnant women, 5%- • 25% • Illness severity: Increased with age • Chronic sequelae: None identified
Hepatitis E Virus Infection Typical Serologic Course Symptoms ALT IgG anti-HEV IgM anti-HEV Titer Virus in stool 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Weeks after Exposure
Hepatitis E - Epidemiologic Features • Most outbreaks associated withfecally contaminated drinking water • Minimal person-to-person transmission
Prevention and Control Measures for Travelers to HEV-Endemic Regions • Avoid drinking water (and beverages with ice) of unknown purity, uncooked shellfish, and uncooked fruit/vegetables not peeled or prepared by traveler • IG prepared from donors in Western countries does not prevent infection • Unknown efficacy of IG prepared from donors in endemic areas • Vaccine?
Hepatitis B - Clinical Features • Incubation period: Average 60-90 days • Range 45-180 days • Clinical illness (jaundice): <5 yrs, <10%³5 yrs, 30%-50% • Acute case-fatality rate: 0.5%-1% • Chronic infection: <5 yrs, 30%-90%³5 yrs, 2%-10% • carrier state (350m ) • Premature mortality fromchronic liver disease: 15%-25%
Acute Viral Hepatitis Source: CDC
Baruch Blumberg, 1963: ‘Australian antigen - Au'. 1967: Au was a viral antigen = HBsAg (surface antigen) Dane, 1970: Discovered 42nm 'Dane particles‘ HBcAg (core antigen). 1973: HBeAg discovered (endogenous antigen = a truncated version of HBcAg). secreted sphere hepatitis B virion secreted filament
spherical, • enveloped (? lipid-containing, detergent disrupted ?) • 42-47nm diameter • d/s DNA • an RNA-dependent DNA polymerase (i.e. reverse transcriptase) • family Hepadnaviridae
HBV genome organization two uneven strands of DNA: (-)sense strand: 3.0 - 3.3kb (+)sense strand: 1.7 - 2.8kb
Reverse transcription P protein Capsid protein ER/IC e Golgi cap RNA pregenome RNA ccc-DNA Precore, L, M, S + X proteins The HBV infectious cycle ( ( (
four open reading frames (ORFs) : S,C,P,X • S – HBsAg • C – HBcAg C + preC – HBeAg • P – polymerase • X – HBxAg (a transcriptional transactivator)
HBsAg & anti-HBs • HBsAg is an envelope protein & an poor immunogen -------- replication • recovery of acute HBV infection is characterized by HBsAg/anti-HBs seroconversion • passively acquired anti-HBs protects individuals from infection with HBV • Anti-HBs is not strictly a ‘neutralizing’ antibody
HBcAg & anti-HBc • HBcAg is not detectable in the sera of some patients. • immunogen • IgM anti-HBc – virus replication, acute infection, transient response • IgG anti-HBc – do not protect individuals, chronic infections, alst for a long time
HBeAg & anti-HBe • HBeAg is produced when virus is replicating. • HBeAg is correlated strongly with the detection of viral DNA, virons and the viral DNA polymerase in the serum. • The disappearace of HBeAg and replacement with anti-Hbe indicates that the patient is responding to the infection and will clear HBsAg.
Acute Hepatitis B Virus Infection with Recovery Typical Serologic Course Symptoms anti-HBe HBeAg Total anti-HBc Titer anti-HBs IgM anti-HBc HBsAg 0 4 8 12 16 24 28 32 52 100 20 36 Weeks after Exposure
Progression to Chronic Hepatitis B Virus Infection Typical Serologic Course Acute (6 months) Chronic (Years) HBeAg anti-HBe HBsAg Total anti-HBc Titer IgM anti-HBc Years 0 4 8 16 20 24 28 36 12 32 52 Weeks after Exposure
Hepatitis B Lab Tests (1) • HBV: Hepatitis B virus. • HBsAg: Hepatitis B surface antigen. Marker of infectivity when found in serum. • anti-HBs: Antibody to HBsAg. Marker of immunity when found in serum. • HBcAg: Hepatitis B core antigen. No commercial test available for this. • anti-HBc: Antibody HBcAg. Marker of past or current infection.
Hepatitis B Lab Tests (2) • IgM anti-HBc: IgM is an antibody subclass of anti-HBc. Indicates recent infection with HBV (<4-6 mos.). • IgG anti-HBc: IgG is a subclass of anti-HBc. Indicates “older” infection with HBV. • HBeAg: Hepatitis B “e” antigen. Can only be present if HBsAg is positive. Marker of high degree of infectivity. • Anti-HBe: Antibody to “e” antigen. May be present in infected or immune person.
Interpretation of Hepatitis B Panel HBsAg negative antiHBc negative susceptible antiHBs negative HBsAg negative antiHBc positive immune due to natural infection antiHBs positive HBsAg negative antiHBc negative immune due to vaccine antiHBs positive HBsAg positive antiHBc positive acutely infected IgM antiHBc positive antiHBs negative HBsAg positive antiHBc positive chronically IgM antiHBc negative infected antiHBs negative HBsAg negative antiHBc positive four possible interpretations antiHBs negative (see next slide)
Four possible interpretations of isolated antiHBc positive 1.May be recovering from acute HBV infection. 2.May be distantly immune and test not sensitive enough to detect very low level of anti-HBs in serum. 3.May be susceptible with a false positive anti-HBc. 4.May be undetectable level of HBsAg present in the serum and the person is actually a carrier.
Concentration of Hepatitis B Virus in Various Body Fluids Low/Not High Moderate Detectable blood semen urine serum vaginal fluid feces wound exudates saliva sweat tears breastmilk
Main Ways to Get Hepatitis B Having sex without condoms with someone who has hepatitis B 1 Sexual 2 Being born to a mother who has hepatitis B Perinatal Sharing needles and syringes 3 Parenteral You can pass hepatitis B to others if you have just gotten the virus (acute hepatitis) or if you are a carrier of the virus (chronic hepatitis).
How does a baby get hepatitis B from mother? • If you have hepatitis B and a tiny bit of your blood gets inside your baby at birth.
Passive immunization Hyperimmune hepatitis B immunoglobulin HBIG Active immunization Vaccine HBsAg CONTROL
1 2 3 Hepatitis B can be prevented! If you have never had hepatitis B,you can get 3 shots . . . . . . and get long lasting protection.
Baby Shots for Hepatitis B if the mother has Hepatitis B 1 - 2 months old Birth + Hepatitis B Vaccine Hepatitis B Vaccine H-BIG 6 months old Hepatitis B Vaccine
Hepatitis D (Delta) Virus d antigen HBsAg RNA
Hepatitis D - Clinical Features • Coinfection • severe acute disease • low risk of chronic infection • Superinfection • usually develop chronic HDV infection • high risk of severe chronic liver disease
Hepatitis D Virus Modes of Transmission • Percutanous exposures • injecting drug use • Permucosal exposures • sex contact
Hepatitis D - Prevention • HBV-HDV Coinfection • Pre or postexposure prophylaxis to prevent HBV infection • HBV-HDV Superinfection • Education to reduce risk behaviors among persons with chronic HBV infection
Hepatitis C Flaviviridae