Download
1 / 30
320 likes | 518 Vues
A social answer to the antisocial behavior of forensic patients. Cognitive Behavioral Therapy, Group therapy and Mentalization ; a connection with possibilities? Anne van den Berg, clinical psychologist and psychotherapist. FPC The Rooyse Wissel , the Netherlands

E N D
A socialanswer to the antisocialbehavior of forensicpatients Cognitive Behavioral Therapy, Group therapy and Mentalization; a connection with possibilities? Anne van den Berg, clinical psychologist and psychotherapist. FPC The RooyseWissel, the Netherlands IAFP 2009, Konstanzanne@berg-op.nl
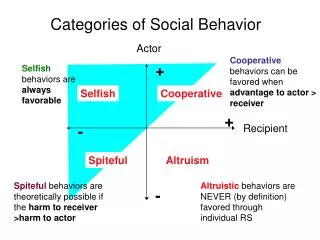
Contents presentation Short overview Dutch forensic psychiatry Cognitive Behavioral Therapy ‘What Works’ principles, advantages and disadvantages Offence Chain Module, advantages and disadvantages Group therapy Mentalization Based Treatment Working apart, together or parallel connected A social answer to antisocial behavior Discussion
A General overview of the Forensicpsychiatry in the Netherlands Cognitive Behavioural Therapy ‘What Works’ principles Risk Guided Focussed on offence relapse prevention Offence chain model Schema Focused Therapy
CognitiveBehaviouraltherapy • dysfunctional emotions, behaviors and cognitions • goal-oriented, systematic procedure • cognitive skills, reducing criminal behavior • monitor thoughts, assumptions, beliefs and behaviors which are dysfunctional, inaccurate, or unhelpful. • replace with more realistic and useful ones. Criticism: no room for irrational feelings and internal conflicts
‘What Works’ principles D.A. Andrews and J. Bonta. The psychology of criminal conduct Research Findings by Meta-Analysis Risk Principle Need Principle Responsivity Principle Integrity Principle
Risk Principle Target those offender with higher probability of recidivism Provide most intensive treatment to higher risk offenders Intensive treatment for lower risk offender can increase recidivism Risks as detailed as possible
NeedPrinciple By assessing and targeting criminogenic needs for change, therapists can reduce the probability of recidivism Criminogenic Non-Criminogenic Anti social attitudes Anxiety Anti social friends Low selfesteem Substance abuse Creative abilities Lack of empathy Medical needs Impulsive behavior Physical conditioning
ResponsivityPrinciple Barriers in contact: - lack of motivation, - anxiety, - intellect - the quality of the therapist, the team and setting
IntegrityPrinciple Don’t drift program Treatment or instrument non-compliance. Don’t reverse the program.
Criticismon ‘What Works’ Suggestion of a new way of thinking and treatment Good Lives Model (T.Ward) No connection with the intra-psychic often irrational world of (forensic) patients Is is principally a research based model and not a therapeutic model
OffenceChain Model Meet the requirements of the ‘What Works’ model Far and wide used in the Forensic Care, especially in the high security hospitals like the TBS Originally developed in the addiction care
Parts of the totaloffencechain model 5 Phases: • Life lines with a cognitive case conceptualisation diagram • Offence scenario • Offence chain • Relapse prevention plan • Offence presentation 6 patients in group. All results projected on screen with laptop and beamer
Offence scenario Describe the offence in details: -the circumstances, -the behavior, -the thoughts, -feelings from 6 hours before the offence, during the offence till 6 hours after the offence.
Offencechain The personal factors leading to offence: - the traits of the offender, - circumstances, - sensitivities, - fallacies, - incentives, - getting out of balance, - pitfalls, - high risk situations, - planning and committing the crime - the effects afterwards Dynamic offence theory
Relapseprevention plan How the patient can prevent in time the steps to committing a crime? Factors in the offence chain: How to handle? • thinking in an other more constructive way • stabilizing by doing more healthy things • structuring your life • coping strategies A lot of alternative behavior applied on the personal situation of the patient
Presentation of the wholeoffencechain Powerpoint presentation by patient: - from life-lines till relapse prevention • to the multidisciplinary team • familiar patients, friends and relatives The meaning: • manifest results what he has learned • public confession about his wrong doing and positive plans
Advantagesoffencechain model Risks are clear Needs behind the offence are clarified Structure and tasks for patients stimulate the self activation The matter is logically and to understand Grip to use alternative behavior in the relapse prevention Good cognitive insight with connections to feelings, development
Disadvantages (1) Individual therapy in the group by way of the screen. Patient’s don’t learn with each other but about each other. Patient’s speak about their offences Patients can use this model as a list to tick of the items By focussing on the past there is a neglecting of the present Premise: offences are committed by losing one’s balance.
Disadvantages (2) Therapist is too much focused on the explicit offence material Therapist is focused on the content and not on the relation between therapist and patient No attention to what a group makes successful (Yalom). Encourages defences
Core of the matter The process of the offence chain group encourages that behavior in terms of content which it want to break down. A classic example of a paradox
How to resolvethis paradox? Healthy balance between: • Content and process level • Attention for the past and the present • Explicit and implicit interventions • Individual, interactional and group interventions
Contributionby Group therapy Recognition of behavioral patterns in the social Microcosm of the group Space for the correctional emotional experience Connecting the destructive forces in the group with the constructive ones.
What is mentalizing? Mentalizing is the ability to see one’s own behaviour and that of others in terms of motives and intentions. To develop the ability to reflect and mentalize, a safe attachment with the caretaker (later on between patient and therapist) is necessary.
MentalizationBasedTreatment (1) 1.ensuring that the patient is able to regulate the attention in therapy to the self or others. 2.ensuring that the patient can deal with the affects within the therapeutic relationship, 3.discussing the affects in the present time 4. discussing how these play a role towards attachment figures in the present and past. 5. encouraging the patient to verbalize his own intentions and those of others; Summary of MBT:
To a combined and social model Starting point: Join the forces of the different point of views but bring no confusion in one group. Solution: 1. Life-lines individual in a more diagnostic framework. Patterns and Schema’s 2. Presentation about life lines as a start in a closed group 3. Three kinds of groups which operate separately but connected in time, in therapists and in theme’s
Three parallel groups Cognitive behavioral group about offence chain and relapse prevention with an attitude of the therapists ‘keeping tot the point’. Group dynamic therapy with more interactional themes in the here and now with space for corrective emotional experience. More process and space for positive feelings and intentions. Elements of MBT therapy. Non-verbal therapies like drama, creative, psychomotor for the more implicit interventions. MBT elements
Finally It is very important to revalue the imperfect clinical experiences of the therapists and those of the patients in stead of, first to all, to trust in the imperfect results of empirical research. Research is for checking your professional person as an instrument. This is a social solution and answer as a counterforce for patients with antisocial behavior like those with ASPD
Experiences? Are there any experiences with combining CBT, group therapy and MBT? How are those experiences? Thank you for your attention!!!! Information: anne@berg-op.nl