Download
1 / 18
180 likes | 294 Vues
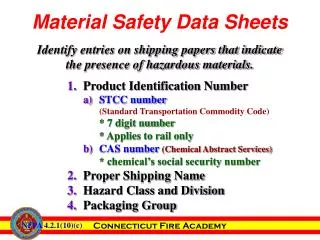
Use of Safety Monitoring Flow Sheets. Background. Flow sheets can serve as useful tools Not required but recommended Tailor for ease of use AND usefulness at your site When tailoring, consider staff roles and responsibilities AND other documentation requirements at your site. Flow Sheets.

E N D
Background • Flow sheets can serve as useful tools • Not required but recommended • Tailor for ease of use AND usefulness at your site • When tailoring, consider staff roles and responsibilities AND other documentation requirements at your site
Flow Sheets • Height and weight • Vital signs • Hematology • Liver function: ALT and AST • Renal function: phosphate and creatinine
Common Elements • Title • Brief instructions/guidance • Date and visit code • Values being monitored • Staff Initials • Shading indicates “not applicable”
General Instructions for Use • Initiate use during screening • File for “easy access” in participant study notebook • Update at or after each visit • Continually review as part of ongoing safety monitoring • Initial and date to document reviews
Height • Why are there two rows to record height on each date?
Height • Because the protocol requires repeat measurement if a decrease of 3.8 cm or more is identified • Record NA if a second measurement is not required and therefore is not done • Severity grading is not required
Weight • Why is percentage difference from Screening Part 2 needed?
Weight • Because the severity of unintentional weight loss must be graded in terms of percent decrease 01 JAN 2010 07 JAN 2010 15 APR 2010 6.0 (M3) 50 50 45 50 – 45 = 5 5 10% 5 ÷ 50 = 0.10 = 10%
Vital Signs • Fever (oral temp), hypertension, and hypotension must be graded • For hypertension, grading requires repeat blood pressure measurement at the same visit
Hematology • Hemoglobin, platelets, white blood cells, neutrophils, and lymphocytes must be graded • Hemoglobin is graded based on absolute values and difference from Screening Part 1 • Neutrophils and lymphocytes are graded based on absolute counts • Although not recorded on flow sheet, abnormal differential counts should also be monitored for clinical significance
ALT and AST • All results should be graded • Grading is based on the site upper limit of normal (record at top of flow sheet for ease of reference)
Phosphate • All results should be graded • Grading is based on the site lower limit of normal (record at top of flow sheet for ease of reference)
Creatinine • Absolute levels must be graded (based on site upper limit of normal) • Increases from baseline must be calculated to determine whether product hold is required • Creatinine clearance rate must be calculated to determine whether product hold is required
Creatinine: Relative Increase From Baseline • Participant is a 23 year old, 57 kg woman, oral study product 1.5 mg/dL 0.8 mg/dL 01 JAN 2010 15 APR 2010 6.0 (M3) 0.8 mg/dL 0 0.9 mg/dL 0 1.1 0.9 ÷ 0.8 = 1.1 99 mL/min 87 mL/min
What are your … • Questions? • Comments? • Concerns?