Download
1 / 73
880 likes | 1.68k Vues
Guillain-Barre Syndrome. Presentor : Izaskun C. Ganao Moderator: Dr. Mary Katherine E. Millan-Morales Reactor: Dr. Teresita N. Rabanal. Objectives. To discuss the approach to a patient with Guillain- Barre Syndrome

E N D
Guillain-Barre Syndrome Presentor: Izaskun C. Ganao Moderator: Dr. Mary Katherine E. Millan-Morales Reactor: Dr. Teresita N. Rabanal
Objectives • To discuss the approach to a patient with Guillain-Barre Syndrome • To discuss the clinical presentation and management of Guillain-Barre Syndrome
IDENTIFYING DATA • JSS • 4 year old • Male • Filipino • From Mandaluyong • Admitted for the 1sttime in our institution last September 30 2013
Chief Complaint Vomiting And Doubling of Vision
History of Present Illness 1 day PTA Patient complained of doubling of vision noted to have inward deviation of the eyes, L>R (-) vomiting (-) history of trauma (-) headache (-) dizziness (-) body weakness (-) seizure Spontaneous resolution of symptoms
History of Present Illness Morning PTA doubling of vision associated with inward deviation of the right eye (+) 4 episodes of vomiting (-) body weakness (-) headache (-) numbness Consult at TMC-ER Advised admission
Review of Systems • Skin(-) jaundice, (-) active dermatoses, (-) pruritus, photosensitivity • Eyes(-) lacrimation, (-) preferential gaze, (-) strabismus, (-) blurring of vision, lacrimation, redness • Ears:(-) discharge, (-) tenderness, (-) ear pain, deafness, tinnitus • Nose: (-) epistaxis, (-) discharge • Mouth: (-) sores, fissures, bleeding gums • Neck: (-) stiffness, limitation of motion on the neck • Pulmonary: (-) hemoptysis, (-) difficulty of breathing • Cardiac: (-) chest pain, orthopnea, syncope • Gastrointestinal: (-) constipation (-) hematochezia , (-) melena • Genitourinary: (-) urgency, hesitancy, dysuria, hematuria, frequency • Muscular: (-) swelling, (-) trauma, (-) wasting • Hematopoietic: (-) bleeding, (-) easy bruising • Endocrine: (-) polydipsia, polyuria, polyphagia, nocturia, (-) heat intolerance tremors • Neuro: (-) headache, seizure, head trauma
Past Medical History • (+) Skin Asthma • (+) Measles – 2011 (2 years old) • No previous head trauma • No known allergies • No previous surgeries • Newborn screen – normal
Family History • (+) Asthma • (+) Diabetes
Birth History • Full term • Normal spontaneous delivery • 31 year old G1P1 (1001) • Birth weight: 2.8 kg • No feto-maternal complications
Nutritional History • No particular food preferences • No known food allergies
Immunization History • BCG - 1 dose • DPT/OPV - 3 doses + 2 boosters • HiB- 3 doses • Hepatitis-B - 3 doses • MMR - 2 doses • Varicella - 1 dose • PCV - 3 doses • Hepatitis - 2 doses • Typhoid - 1 dose • Influenza – Last dose: 2012
Physical Examination at the ER • General survey – Awake, active, not in cardio-respiratory distress • Vital signs: BP: 90/60 CR: 82 bpm RR: 26 cpm T: 36.1⁰C Weight: 16 kg Height: 105 BMI: 14.5
Physical Examination at the ER • Nonsunken eyeballs, moist lips, no oral sores • Symmetrical chest expansion, no retractions, clear breath sounds • Adynamic precordium, normal rate, regular cardiac rhythm, no murmurs • Flat abdomen, normoactive bowel sounds, soft abdomen, nontender • Full pulses, CRT less than 2 seconds, warm extremities
Physical Examination at the ER • Neurologic Examination • GCS 15, awake, follows commands, coherent, able to speak and comprehend spoken language
Cranial nerves: • CN I – intact • CN II, III – pupils equally briskly reactive to light • CN III – no ptosis, pupils equally briskly reactive to light • CN IV – no diplopia on looking down or in • CN VI – diplopia on lateral gaze to the right • CN V – intact corneal reflex • CN VII – no facial asymmetry • CN VIII – intact gross hearing • CN IX, X - can swallow, intact gag • CN XI – good shoulder shrug • CN XII – tongue midline
Physical Examination at the ER • Neurologic Examination • CN V – intact corneal reflex • CN VII – no facial asymmetry • CN VIII – intact gross hearing • CN IX, X - can swallow, intact gag • CN XI – good shoulder shrug • CN XII – tongue midline
Physical Examination at the ER • Neurologic Examination Motor: Sensory: Deep tendon reflexes:
(-) Babinski • (-) Clonus • Supple neck, non meningeal signs
Admitting Impression Vomiting, unspecified; t/c abduction deficit, OD more than OS, probably secondary to cranial nerve VI compression ; R/O Intracranial mass
Therapeutics: • Eye patch application for 4 hours each eye alternately • Vitamin B complex once a day
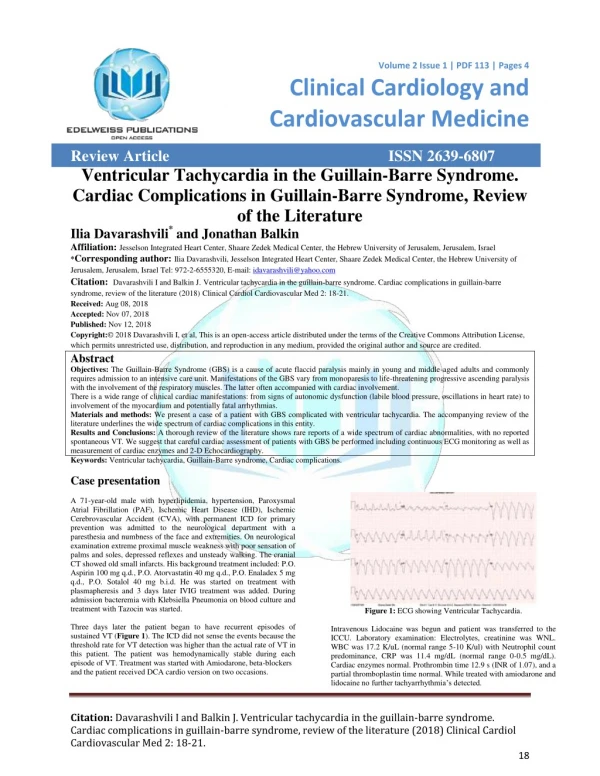
Laboratory Examinations • HGT: 102 mg/dL • ECG: sinus bradycardia, normal sinus rhythm • Chest x-ray: no significant chest findings • MRI of the orbits: polysinusitis, enlarged adenoids, unremarkable MRI of the orbits
Laboratory Examinations • EMG-NCV of the lower extremities: normal findings for age except for the bilateral absence of the H-reflex. Consider beginning or early polyneuropathy.
Laboratory Examinations • Electromyography/Nerve conduction Study of the lower extremities • normal findings for age except for the bilateral absence of the H-reflex • Electrical equivalent of the tendon jerk • ECG • sinus arrhythmia
Final Diagnosis Guillain-Barre Syndrome, Miller-Fisher Variant; s/p IVIg; Polysinusitis
Salient Features • 4 year old male • Afebrile • Doubling of vision • Vomiting • Abdominal pain • Constipation • Ascending weakness of the extremities • Areflexia of the lower extremities • Limitation of movement of extraocular muscles • Arrhtyhmia and bradycardia • Ptosis • Headache • Difficulty swallowing liquids • Hoarseness of the voice
Intracranial mass • headache, • altered mental status • ataxia • nausea, vomiting • weakness, and gait disturbance • focal seizures • fixed visual changes • speech deficits • focal sensory abnormalities
Botulism • Nausea • Vomiting • Extremely dry mouth unrelieved by drinking fluids • Sore throat • Cranial nerve paralysis manifesting as: • blurred vision • diplopia • Ptosis • extraocularmuscle weakness or paresis • fixed/dilated pupils • dysarthria • dysphagia or suppressed gag reflex
Botulism • Paralytic ileus advancing to severe constipation • Gastricdilatation • Bladder distention advancing to urinary retention • Orthostatic hypotension • Reduced salivation • Reduced lacrimation
Botulism • Changes in deep tendon reflexes, which may be either intact or diminished • Incoordination due to muscle weakness • Absence of pathologic reflexes and normal findings on sensory and gait examinations • Normal results on mental status examination
Botulism • Symmetrical descending paralysis or weakness of motor and autonomic nerves • Respiratory muscle weakness subtle or progressive, advancing rapidly to respiratory failure
Poliomyelitis • Fever • Headache • Nausea/Vomiting • Abdominal pain • Oropharyngealhyperemia • Nuchal rigidity • Back and lower extremity pain • Meningitis with lymphocytic pleocytosis (usually) Paralytic poliomyelitis occurs in fewer than 5% of affected patients and is characterized by the following: • Compromise of the motor neurons may be localized or widespread. • asymmetric loss of muscle • Muscle atrophy is generally observed several weeks after the beginning of symptoms.
Myasthenia Gravis • specific muscle weakness rather than generalized muscle weakness • The severity of the weakness typically fluctuates over hours being least severe in the morning and worse as the day progresses • increased by exertion and alleviated by rest • The degree of weakness also varies over the course of weeks or months, with exacerbations and remissions • Extraocular muscle weakness or ptosis is present initially in 50% • Patients progress from mild to more severe disease over weeks to months. • Weakness tends to spread from the ocular to facial to bulbar muscles and then to truncal and limb muscles