Download
1 / 14
140 likes | 537 Vues
Diabetic retinal screening in Shetland. An over view of the local service Kathleen Carolan, April 2006. Why has the diabetic retinopathy screening programme been developed?. Diabetic retinopathy is the major cause of blindness in the 30-65 age group in the UK at the present time.

E N D
Diabetic retinal screening in Shetland An over view of the local service Kathleen Carolan, April 2006
Why has the diabetic retinopathy screening programme been developed? • Diabetic retinopathy is the major cause of blindness in the 30-65 age group in the UK at the present time. • Regular (annual) screening for retinopathy detects those at risk before visual symptoms occur and when treatment outcome is optimal. • Treatment can prevent blindness in 90% of those at risk if applied early and adequately • It is a requirement of all Health Boards in Scotland that an accredited DRS service is in place and available to all eligible patients.
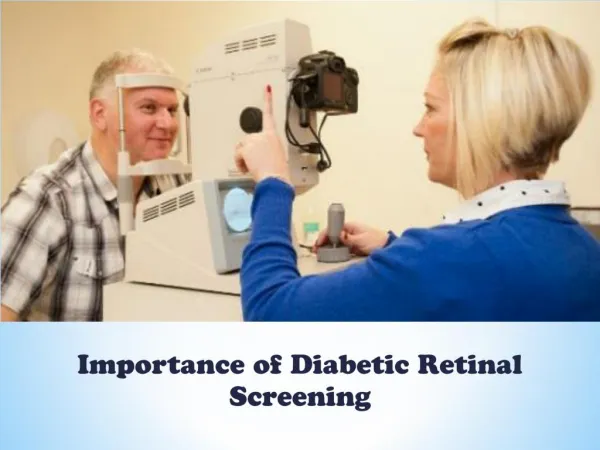
What happens at the screening examination? • Digital images are taken using a fundus camera. • The procedure (taking the images) is painless. • If the patient has small pupils – then drops will be instilled to dilate the pupils. This can make the eyes water/stings. • Eye drops mean that the patient cannot drive/operate machinery for up to 6 hours after the screening (due to blurred vision). • Patient leaflets are sent out with the invite letter to tell them about the screening and possibility of drops.
Results Dispatch Results are dispatched to the patient, Practice & diabetic clinic. Onward referrals for ophthalmology sent to Information Dept for booking into next available visiting clinic Patient Focussed Booking Rebook patient for recall at the specified time (e.g. 12/12, 6/12 etc) GP Practice Asked to look at all diabetic patients on GPASS – and forward a register of all eligible patients to Kathleen Carolan Patient Focussed Booking Kathleen provides patient details to the booking service. Patients are offered an appointment/transport arranged etc. Grampian return results via email 4-8 weeks after screening Screening Images Sent to Grampian Screening operator post processes images and emails to ARI for grading/reporting Patient Focussed Booking Generates a clinic list for the screening operator Screening Operator Screens patients & notifies PFB about DNAs, dilated patients, special arrangements for recall in the future so that it can be logged on the DRS master register If new patients are diagnosed these details are forwarded to KC DRS service – current process for administration management
Photography error – rebook appointment with the local screener Images are sent via email to the Regional Unit in Grampian for grading (reporting on) Technical failure – book appointment with visiting ophthalmologist for slit lamp examination. FURTHER APPOINTMENTS & RECALL INSTRUCTIONS Results are emailed back to Kathleen Carolan for distribution & onward referral (usually received 4-6 weeks after screening) Retinopathy detected. No retinopathy detected = recall in 12 months. Mild background = recall in 12 months. Moderate background = recall in 6 months. Observable = recall in 6 months. Maculopathy = needs an ophthalmology appt within 4 months. Severe background = Shetland Ophthalmology appt within 3 months. Early proliferative* = direct referral to ARI within 1 month. High risk proliferative* = direct referral to ARI ASAP. * means at an Aberdeen eye clinic not visiting clinic Pregnant (diabetic) women – screen every 3 months DESTINATION OF REPORTS Report sent to Dr Pauline Wilson and filed in the medical notes Report sent to the GP Practice C/O the Practice Manager & results entered on to GPASS Results letter sent to the patient detailing outcome of the screening & whether onward referral is required DRS service – current process for managing call/recall and onward referral
Recall Booked on SOARIAN Generating clinic lists This will be done in SOARIAN. Because all Shetland patients will be in the system at the same time – patients can be called in any order. GP Practice SCI Network (SCIN) genie installed so that the SCIN system can look directly at GPASS & take patient register for DRS Populating the new national DRS system SCIN will have a link with SOARIAN. This will create a secure Shetland wide register. Onward Referral Remain manual referral process but outcome of eye clinic appt will be stored on SOARIAN. Returning Results The results will be available on SCIN for Practices/Diabetes Clinic staff to act on. Screening Operator All local screening administration will be done in SOARIAN. Practices will be asked to exclude patients on SCIN Benefits– the register will be automatically updated by GPASS every 24 hours. Results will go back directly to the Practice – no rekeying reqd. Screening Images Grampian will pick up the screening images from the SOARIAN system automatically. Reporting Grading Results Grampian graders will enter results directly on to SOARIAN. DRS service – changes to the way we call/recall patients in the future
SCI Network System http://training.diabetes.scot.nhs.uk User name: training Password: train2005
Roll out plan (pre August 2006) • Offer appointments to patient currently not seen in Lerwick, (including 12-18 year olds). • Offer appointments to Levenwick & Scalloway Practices (during May/June/July). • Train HCA to provide 10 screening hours per week (extra capacity to manage programme in Year 1 also reqd). • Look at model for providing ‘one off’ mobile clinic in north mainland to ensure equity of access. • Ensure that all patients are validated and accessible to the SOARIAN system via SCIN.
Roll out plan (post August 2006) • Offer appointments to all remaining patients not seen at previously available mobile and static clinics by March 2007 (this will mean that patients can be offered appointments at their convenience and in any Practice order). • Continue to review capacity (screening/admin time), activity (volume of patients seen) and quality issues (process for DRS) within the service.
For further information • Contact: Kathleen Carolan Tel: 01595 743000 (ext 3188) Kathleen.carolan@shb.Shetland.scot.nhs.uk