Download
1 / 37
510 likes | 1.33k Vues
Early Gastric Cancer. Dr. LF Hung Department of Surgery, Tuen Mun Hospital, HKSAR. Background. In 2005 1028 new cases of gastric cancer in Hong Kong 5 th commonest cancer 4 th major cause of cancer deaths (635). Early Gastric Cancer (EGC). Definition:

E N D
Early Gastric Cancer Dr. LF Hung Department of Surgery, Tuen Mun Hospital, HKSAR
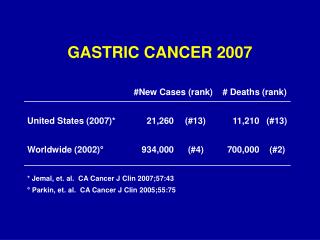
Background • In 2005 • 1028 new cases of gastric cancer in Hong Kong • 5th commonest cancer • 4th major cause of cancer deaths (635)
Early Gastric Cancer (EGC) • Definition: • gastric cancer confined to the mucosa or submucosa, regardless of the presence or absence of lymph node metastasis (T1) • In Japan • ~50% patients with gastric cancer present as EGC • Mean age : 55 • In Western countries: • ~ 15% patients with gastric cancer present as EGC • Mean age : 63
Tuen Mun Experience • A retrospective study for the outcome of early gastric cancers from Jan 1999 to June 2006 in TMH • Data was collected from hospital computer records • All patients with operations done for gastric cancers were included • Diagnosis of EGC was confirmed by histology • Survival was analyzed with Kaplan Meier Curves • Cox regression was performed to analysis the predictive factors for survival
TMH figures • 298 operations for gastric cancers from Jan 1999- June 2006 in TMH
Early gastric cancers • 38 cases of early gastric cancer • All operations for EGC were performed with curative intention
Demographic Data – age • Median age 72
Demographic Data – sex ratio ~ ¾of EGC patients are male
Common Presenting symptoms • Epigastric pain 53% • Upper GIB 34% • Anaemia 18% • Weight loss 5%
Cancer-specific survival • 5 yr-survival 88.9%
Causes of deaths • 2 deaths due to tumor recurrence • 1 early post-operative deaths • Duodenal stump leakage
Potential predictive factors • Age • Sex • Tumor location • Type of operation • T stage • N stage • No. of metastatic LN • No. of LN yielded • Cell type • Degree of differentiation
Cox regression – EGC overall survival • Age is the only significant predictive factor ( p= 0.001) • Other predictive factors are not significant • Older ageis associated with medical co-morbidities
Japanese study • British Journal of Surgery 2004 • 4231 patients with EGC studied • Overall survival rate and cause of death analysed
Results • 5- and 10-year cancer-specific survival rates were 98.4 and 96.3 • Overall survival rates were 90.2 and 80.9 % • The critical age for determining prognosis was 70 years for men and 75 years for women • Age identified as the most powerful prognostic indicator in EGC
Treatment for EGC • Traditionally: • Radical surgery with extended lymphadenectomy (D2 dissection) • Excellent 5 year survival, > 90% • Incidence of positive nodes in: • mucosal GC: 1.8% - 5% • submucosal GC: 10%-25% • EGC rarely spreads beyond the perigastric nodes • Question: Is uniform radical surgery and D2 dissection always necessary ?
Treatment for EGC • Post-gastrectomy morbidity: • Early and late dumpling syndrome • Reflux esophagitis • Alkaline regurgitation • Weight loss • Malabsorption • Vitamin and mineral deficiency • Anaemia • Metabolic bone disease
Treatment for EGC • Current surgical trend: • Extensive resection Tissue preservation • Uniform performance Individual basis • Minimizing morbidity and mortality • Maximizing therapeutic effects and quality of life • Tissue preservation: • “reduced” scope of lymphadenectomy • “reduced” resection of the stomach • concept of : “less invasive” surgery
Current Treatment Strategies • Reduced resection of stomach: • Endoscopic resection (EMR/ESD) • Pylorus preserving gastrectomy • Proximal gastrectomy • Laparoscopic gastrectomy • Reduced scope of lymphadenectomy: • Modified D1 dissection • Modified D2 dissection
Endoscopic mucosal resection • Endoscopic mucosal resection (EMR) for EGC: • currently standard practice in Japan • less invasive and more economical • cure can be accomplished by local treatment in selected cases • allows complete pathological staging of the cancer • Accepted indications for EMR are: • (1) well-differentiated elevated cancers less than 2 cm in diameter • (2) small depressed lesions (<1cm) without ulceration
Indication for EMR • Prediction of lymph node metastasis: • Lesion < 2 cm size • Well or moderately differentiated histology • No macroscopic ulceration • Invasive disease limited to mucosa and not deeper than superficial submucosa • No lymphovascular invasion • If criteria are met: lymph node metastasis exist in only 0-4% of patients
EMR in EGC • A) The inject and cut technique. • B) The inject, lift, and cut technique • C) EMR with cap-fitted panendoscope • D) EMR with ligation
EMR in EGC • Limitation of EMR: • cannot be used to resect lesions > 15 mm in one piece • piecemeal resection specimen are difficult for pathological analysis, causing inadequate staging • high risk of recurrence (up to 35%) • Endoscopic submucosal dissection (ESD), method of en-bloc resection developed
Endoscopic Submucosal Dissection • provides en-bloc specimens • precise histological staging and may prevent disease recurrence • requiring significant additional technical skills • longer procedure time
ESD in EGC • Commonly used devices: • insulation-tipped diathermy knife (IT knife) • hook knife • flex knife
Proposed extended criteria for endoscopic resection T. Gotoda 2007
Complications of endoscopic resection • Pain • Bleeding: • EMR: 8% • ESD: 7% • Managed by hot biopsy forceps or bipolar haemostatic forceps • Perforation: • Uncommon in EMR • ESD: 4% • Closed with endoclips
Local resection (EMR/ESD) • Advantage: • Offer best quality of life • Excellent disease specific survival • Disadvantage: • Local recurrence when resection margin not clear
Current Treatment Strategies • Reduced resection of stomach: • Local resection • Pylorus preserving gastrectomy • Proximal gastrectomy • Laparoscopic gastrectomy • Reduced scope of lymphadenectomy: • Modified D1 dissection • Modified D2 dissection
Laparoscopic gastrectomy • Laparoscopic assisted Billroth I Gastrectomy (Kitano 1991) • Total laparoscopic, laparoscopic assisted, hand-assisted gastrectomy • Standard D2 LN dissection is technically feasible
Laparoscopic gastrectomy • Better short term outcome compared with open gastrectomy : • decreased pain • improved pulmonary function • early recovery of bowel function • shorter hospital stay • Comparable oncological clearance • Comparable long term survival
Laparoscopic gastrectomy • Technically demanding • Need multicenter RCT to validate the short term and long term outcome results
Conclusion • Routine radical surgery + lymphadenectomy in early gastric cancer may carry significant morbidity and possible mortality • Practice of “less invasive” procedure can: • Maintain same therapeutic efficacy • Improve patient quality of life