Download
1 / 37
390 likes | 728 Vues
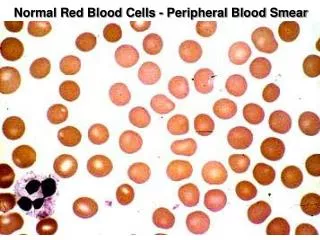
Seeing is Believing: The Importance of the Peripheral Blood Smear. Marc J. Kahn, MD , MBA, FACP Peterman-Prosser Professor Sr. Associate Dean Tulane University School of Medicine New Orleans, LA. Case 1.

E N D
Seeing is Believing: The Importance of the Peripheral Blood Smear Marc J. Kahn, MD, MBA, FACP Peterman-Prosser Professor Sr. Associate Dean Tulane University School of Medicine New Orleans, LA
Case 1. A 42 year old African American presents to his primary care provider for colicky abdominal pain of three weeks duration. US reveals multiple gallstones. His peripheral smear is shown.
What is the diagnosis? A. Sickle cell disease B. SC disease C. Hereditary elliptocytosis D. Southeast Asian ovalocytosis
Hereditary elliptocytosis • Not typically anemic • Often noted incidentally • Can form pigment gallstones • Abnormality in red cell scaffolding—ankyrin, spectrin, protein 4.1 etc.
Case 2. A 72 year old man is noted to be pale and complains of dyspnea on exertion of 3 weeks duration. His pulse is 112 with a blood pressure of 120/70. He has pale conjunctivae. He has no organomegaly or adenopathy. His hgb is 6.2 g/dl. His peripheral smear is shown
What is your diagnosis? A. Iron deficiency B. Alpha thalassemia trait C. Autoimmune hemolytic anemia D. Folate deficiency E. Hgb SC disease
Warm antibody hemolytic anemia • spherocytes • Coomb’s positive IgG • May be due to underlying lymphoproliferative disorder • Hemolysis occurs in spleen
Case 3. A 25 year old man is being evaluated for an anemia found on routine screening. He has been told that he was anemic since birth. His hgb is 10.2 g/dL with an MCV of 65 fL. His erythrocyte count is 5.9 million. His peripheral smear is shown
What is your diagnosis? A. Beta thalassemia minor B. Iron deficiency C. Cold agglutinin disease D. Hereditary spherocytosis E. G6PD deficiency
Beta thalassemia minor • Target cells • Low MCV with preserved or elevated RBC count • Metzner index: MCV (fL)/RBC count (million) • >13 = iron deficiency • <13 = thalassemia
Case 4. A 35 year old woman is being evaluated for a chronic anemia. Her hgb runs in the 9-10 g/dL range. She has had a cholecystectomy in the past and is otherwise healthy. Her peripheral smear is shown:
What is your diagnosis? A. Sickle cell disease B. Hgb C disease C. Hereditary elliptocytosis D. G6PD deficiency
Hgb C disease • Point mutation in beta chain • Precipitated Hgb C seen on smear • No painful crisis • Hgb electrophoresis can help with diagnosis
Case 5. A 22 year old woman has had chronic ITP for several years. She has been treated with prednisone, splenectomy, rituximab and vincristine in the past without response. Her current platelet count is 42,000. Her peripheral smear is shown
What is your diagnosis? A. Chronic ITP B. Pseudothrombocytopenia C. May Hegglin abnormality D. malaria
May Hegglinabnomality • Congenital • Does not require treatment • Macrothombocytopenia and Dohle bodies • MYH9 mutations
Case 6. A 16 year old boy is a frequent abuser of inhalant drugs. He presents with sudden loss of memory, confusion and lack of coordination. His peripheral blood smear is shown.
What is he likely inhaling? A. glue B. nitrous oxide C. Paint D. hairspray
Nitrous oxide toxicity • Inactivates cobalamin via oxidation • Symptoms can occur quickly • Serum B12 can be normal • Treated with high doses of B12
Case 7. A 72 year old man with a history of COPD is brought into the emergency room with a temperature of 102 F, pulse of 115 and SBP of 70. He is emergently intubated, stabilized and sent to the ICU. His peripheral smear is shown.
What is your diagnosis? A. Pneumococcal sepsis B. Gram negative sepsis C. contaminant
Case 8. Peripheral smear shown
What is your diagnosis? A. Ascaris B. Trypanosomiasis C. Wucheriabancrofti D. Schistosomiasis
Wucheriabancrofti • Filiariasis • Africa, South America • Can lead to elephantiasis if untreated • Mosquito vector
Case 9. • Peripheral smear shown