Download
1 / 17
170 likes | 281 Vues
Improving defaulter rates in Ambulatory Feeding Programs. Ellen van der Velden (Investigator) Saskia van der Kam. June 2008. Background High defaulter rates in ATFP. Objectives.

E N D
Improving defaulter rates in Ambulatory Feeding Programs Ellen van der Velden (Investigator) Saskia van der Kam June 2008
Objectives • Identify key factors modifiable by MSF that would decrease defaulting in ambulatory feeding programs (ATFP)
Methods • Analysis of available quantitative program data • Analysis of qualitative information from interviews and observation (all under program field conditions)
Methods Plus • Some defaulter interviews in South Sudan
Results Quantitative methods • Defaulters do not differ from non-defaulters in terms of • Age • Gender • Weight on admission • Height on admission • Irregular attendance not associated with defaulting • Defaulting occurred regardless of last recorded W/H status
Qualitative methods Behaviour analysed from three perspectives • Personal perception of likely consequences (Behaviour belief) • Social norms (Normative belief) • Personal perception of ability to act (Control belief)
Result Personal and Social Beliefs • Caretakers perceived their child was sick, not malnourished • Caretakers lacked an understanding of the purpose of the nutritional program • Social beliefs/norms have a limited impact on defaulting rates
Results Control Beliefs Security • Insecurity related to traveling was identified as a barrier • Influence of insecurity not measurable Costs • Direct costs (money) seen as low • Indirect costs are considerable (e.g. long waiting time, travel time, opportunity costs)
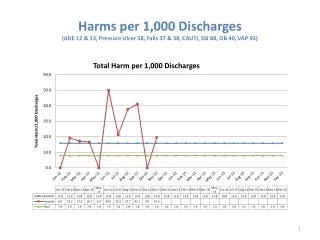
Distance as barrier to completion of treatment % Cured/ defaulter
Limitations of study • Conducted under field conditions while providing technical support to programs • Limited access to beneficiary perspectives
Conclusion Many obstacles identified are modifiable • Mother’s understanding of program aims • Geographical access • Patient waiting times and clinic opening • Food stock ruptures
Recommendations • Improve MSF- caretaker communication (personal and community level) • Outreach indispensable for retention and tracing • Decentralization to increase access • Efficient patient flow
Acknowledgements • Field teams and beneficiary participants in the 5 programs • Royal Tropical Institute (KIT), Amsterdam