Download
1 / 29
290 likes | 735 Vues
Ovarian Stimulation in IUI- Overview. Dr. Jyoti Bhaskar MD MRCOG Director Lifecare IVF. Rationale for COH in IUI. Increasing the number of eggs available for fertilisation Overcoming subtle defects in ovulatory function and luteal phase. Aim of COH. Recruiting multiple follicles

E N D
Ovarian Stimulation in IUI- Overview Dr. Jyoti Bhaskar MD MRCOG Director Lifecare IVF
Rationale for COH in IUI Increasing the number of eggs available for fertilisation Overcoming subtle defects in ovulatory function and luteal phase.
Aim of COH Recruiting multiple follicles Control timing of ovulation Prevention of premature LH surge To time the insemination Increase the pregnancy rate
Optimum Ovarian Stimulation for IUI • 2 – 3 follicles with Ø 18 – 19 mm. • Endometrium 9 mm thick & trilaminar. • IUI between Cycle D13 and D16, 36-40 hrs. from HCG inj.
Classification WHO I - Hypothalamic pituitary failure (Hypogonadotrophic hypogonadism) Kallman’s, Sheehan’s, anorexia II - Hypothalamic pituitary dysfunction (PCOS) III – Ovulatory Failure – Hypergonadotrophic hypogonadism, Turner’s, autoimmune, mumps, RT, CT
Drugs for Ovarian Stimulation Clomiphene Citrate, Gonadotrophins: HMG highly purified ur FSH Rec. FSH GnRH antagonist
CLOMIPHENE CITRATE Most widely Simple to use, Minimal side effects, Cost effective
CLOMIPHENE CITRATE ( SERM) Binds HYPOTHALAMUS ER GnRH Blocks ER Pituitary FSH Cervix Vagina OVARY Endometrium Folliculogenesis
DOSAGE • Single dose -- together • Monitor Cycle with USG • If ovulation confirmed – maintain same dose • Max to 150 mg Starting Dose 100mg day 2 onwards for 5 days
CC FAILURE ( 40%) No Pregnancy 2 CYCLES OF CC WITH OVULATION AND TIMED INTERCOURSE 2 CYCLES OF CC WITH IUI
CC RESISTANCE (20%) 2 CYCLES OF CC NO OVULATION COST , PT’S CHOICE COUNSELLING GONADOTROPHINS CC + GONADOTROPHINS
Antioestrogenic Effect Thin Endometrium Poor cervical Mucus Start early in cycle – Day 2 or Day 1 Add oestradiol valearate from day 8/9 Use all gonadotrophin cycle
Gonadotrophins - Indications CC Resistance CC Failure
HMG Highly purified Urinary HMG/FSH Recombinant. FSH Choice of Gonadotrophins Day 2 LH/FSH FSH WHO group1 LH PCOS FSH HMG
DOSE • BMI • Ovarian reserve • Age • Cause of Infertility • Dose needed in previous cycle
Complications Multifetal pregnancy OHSS - Life threatening Monitoring Experience Strict protocols
CC only with TI or IUI CC ± FSH or ± HMG with IUI Gonadotrophin only Conventional regime Gn. Low dose step-up protocol Gn. step-down protocol 4. Gonadotrophin with GnRH antag Protocols
CC ONLY PROTOCOL -- +/- IUI DAYS OF CYCLE 2 3 4 5 6 7 8 9 10 11 12 13 14 15 21 TVS – ET AND AFC CC 100 MG DAILY Day 2-6 TVS – FOLLICLE SIZE, ET IF ET< 5MM OV 2MG BD DAILY TVS – FOLLICLE , ET , CERVICAL MUCUS STUDY, POST COITAL TEST FOLLICLE >20MM -- LH SURGE + VE-VE Inj HCG 5000 U i/m Timed Intercourse stat 8pm 24hrs later at 8am 36 hrs later at 8am at Lifecare IUI Sexual relation at same night and for 2 days Luteal support – ETV ES/ Susten vaginally at night Serum Progesterone 7 days after IUI/Ovulation B LONG F ONCE DAILY ALL THROUGH OUT THE CYCLE UPT 18 days after IUI/Ovulation
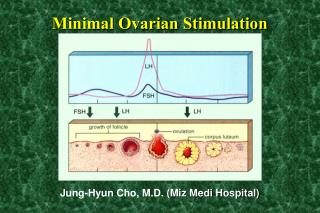
Unripe follicle Ripening follicle Ovulation Corpus luteum Regression of Corpus luteum HCG Oocyte mature 38 hrs Clomiphene 100 mg day2 for 5 days Gonadotrophin stimulation Leading follicle > 18mm
Gonadotrophin Regimens Chronic Low dose Step up regimen 150 IU 112.5 IU hCG 75 IU 37.5 IU Days 7 14 21 28 Step down 112.5 IU 150 IU hCG 75 IU Foll. 10 mm Conventional Regime 75-150 U daily hCG 6 12 Foll. 16mm
Gonadotrophins with Antagonists • Lubek Protocol • French Protocol 15-20% cycles with Gonadotrophins have premature LH surge
Advantages of Antagonist Protocol • Helps avoid IUI at weekends • Compared to agonist – simple and inexpensive • Lower rates of OHSS
Anti-oestrogens Cost effective but less effective when comparedto gonadotrophins. Do not prevent multiple pregnancies Have anti-oestrogeniceffect on the endometrium Gonadotrophins Most effective drugs for IUI Low dose protocols (50 to 75 IU per day) are advised Pregnancy rates do not seemto differ significantly frompregnancyrates with high dose regimens (> 75 IU per day) whereas thechanges to encounter negative effects from ovarian stimulation,such as the risk ofmultiples and the risk ofOHSSmight be higher with high dose protocols. 23 The Cochrane Library 2011, Issue 6 Cantineau AEP, Cohlen BJ
GnRH-agonists There seems to be no role in IUI programs Increase costs Increase multiples without increasing the probability of conception Urinary gonadotrophins versus Recombinant products There is no significant difference GnRH-antagonists Whether or not are going to play a role inmild ovarian hyperstimulation/IUI programs needs to be determined in future trials. Letrozole There is no convincing evidence that Letrozole is superior to clomiphene citrate and therefore the costshould be taken into account when using anti-oestrogens. The Cochrane Library 2011, Issue 6 Cantineau AEP, Cohlen BJ
Ovarian stimulation protocols(anti-oestrogens, gonadotrophinswith and without GnRHagonists/antagonists)for intrauterine insemination (IUI) in women with subfertility (Review) The Cochrane Library 2011, Issue 6 Cantineau AEP, Cohlen BJ Gonadotrophins might be the most effective drugs with IUI Low dose protocols are advised No studies using CC + gonadotrophins 25
There is evidence that IUI with OH increases the live birth rate compared to IUI alone. The likelihood of pregnancy was also increasedfor treatment with IUI compared to TI both in stimulated cycles. There is insufficient data on multiple pregnancies and other adverseevents for treatment with OH. Therefore, couples should be fully informed about the risks of IUI and OH as well as alternative treatment options. 26
Conclusion Choice depends on doctors expertise and patients condition, choice Gonadotrophin only protocol offers the best success rate TIME TO MOVE ON TO TOTAL GONADOTROPHIN CYCLE
Ovarian Stimulation protocol • Simple • Cost Effective • Minimal side effects • Best success rates