Download
1 / 49
1.32k likes | 5.93k Vues
HL. Fun with Shoulder Dystocia. A review of the risks, physiology, management, and prevention of Shoulder Dystocia. Next Slide. Dystocia Introduction. Shoulder dystocia refers to difficulty in delivery of the fetal shoulders.

E N D
HL Fun with Shoulder Dystocia A review of the risks, physiology, management, and prevention of Shoulder Dystocia Next Slide
Dystocia Introduction • Shoulder dystocia refers to difficulty in delivery of the fetal shoulders. • It occurs in 0.2 to 2 percent of births and can be a devastating obstetric emergency. • Some shoulder dystocias can be anticipated and prevented, however, most occur in the absence of risk factors. • Therefore, the obstetrician must be prepared to recognize a shoulder dystocia immediately and proceed through an orderly sequence of steps to effect delivery in a timely manner. • The goal of management is to prevent fetal asphyxia, while avoiding physical injury (eg, Erb's palsy, bone fractures). Next Slide
DEFINITION • Shoulder dystocia can be defined as failure of the shoulders to spontaneously traverse the pelvis after delivery of the fetal head. • In practice, the diagnosis of shoulder dystocia is subjective; it is considered when the routine practice of gentle, downward traction of the fetal head fails to accomplish delivery. Next Slide
PATHOPHYSIOLOGY • The fetal bisacromial diameter normally enters the pelvis at an oblique angle with the posterior shoulder ahead of the anterior one, rotating to the anterior-posterior position at the pelvic outlet with external rotation of the fetal head. Next Slide
PATHOPHYSIOLOGY • The anterior shoulder can then slide under the symphysis pubis for delivery. • If the fetal shoulders remain in an anterior-posterior position during descent or descend simultaneously rather than sequentially into the pelvic inlet, then the anterior shoulder can become impacted behind the symphysis pubis and/or the posterior shoulder may be obstructed by the sacral promontory. • Then you get the dreaded “Turtle Sign” of doom. Next Slide
Turtle Sign More about this in a bit Next Slide
Vignette • Jaquita is a 39 YO AAF G3P2 at 41 6/7 weeks that you have been seeing since her first trimester. The pregnancy has been complicated by gestational diabetes. She has gained 90 lbs during this pregnancy and currently weighs 280 lbs. The Estimated Fetal Weight is 4100 grams. She is a non-smoker. • What are some of her risk factors for Shoulder Dystocia? • Click HERE for answer.
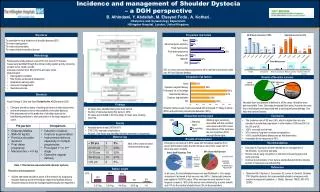
Risk Factors for Shoulder Dystocia • Maternal • Abnormal pelvic anatomy • Gestational diabetes • Post-dates pregnancy • Previous shoulder dystocia • Short stature • Fetal • Suspected macrosomia • Male sex • Labor related • Assisted vaginal delivery (forceps or vacuum) • Protracted active phase of first-stage labor • Protracted second-stage labor Put mouse over chart to review pt’s information. Next Slide
RISK FACTORS • Numerous risk factors for development of shoulder dystocia exist. • One of these risk factors is Fetal Macrosomia. • Jaquita’s Risk factors for fetal macrosomia are listed in Table 1 (show table 1). • Macrosomia has consistently been shown to be one of the major risk factors for shoulder dystocia. • Macrosomia is best defined as: • An estimated fetal weight (EFW) or birth weight >4000 grams • or Birth weight >90th percentile for gestational age (show table 2). • The overall prevalence of birth weight over 4000 grams in the general obstetric population of the United States is 10 percent, but falls to 1.5 percent for birth weight over 4500 grams. Next Slide
Jaquita’s Return to Previous Slide
Return to Previous Slide The EFW for Jaquita’s baby is in the 90th percentile.
RISK FACTORS • The relationship between fetal/newborn size and shoulder dystocia is illustrated by the following: • The incidence of shoulder dystocia increases progressively as birth weight increases over 4000 grams (show table 3). • However, all extremely large infants do not have shoulder dystocia. As an example, a report of 110 infants delivered vaginally with birth weights greater than 5750 grams (12.5 pounds) reported a frequency of 40 percent. • Approximately 50 percent of cases of shoulder dystocia occur in infants whose birth weight is less than 4000 grams. Next Slide
Jaquita’s percent is in the red box. Return to Previous Slide
RISK FACTORS • Unfortunately, it is difficult for the us to identify fetal macrosomia. • One review found that the sensitivity and specificity of ultrasonographic examination to detect fetal weight greater than 4500g were 22 to 69 and 98 to 99 percent, respectively, and the posttest probability of macrosomia after ultrasound diagnosis was only 22 to 37 percent. • EFW using ultrasound biometry did not appear to be substantially more accurate than clinical estimates based upon palpation using Leopold's maneuvers. Next Slide
RISK FACTORS • Diabetes mellitus — Maternal diabetes mellitus increases the incidence of large-for-gestational age (LGA) infants. • Specifically, the chest-to-head and shoulder-to-head ratios are increased in infants of diabetic mothers, thereby increasing the risk of shoulder dystocia independent of fetal weight. • Maternal diabetes mellitus increases the likelihood of shoulder dystocia two to six fold over the nondiabetic population. Next Slide
RISK FACTORS • The correlation between shoulder dystocia and birth weight in diabetic and nondiabetic gravidas is shown in Table 3 (show table 3). • The high rate of shoulder dystocia is associated with a high rate of brachial plexus injury. • The increased risk of shoulder dystocia in diabetic pregnancies occurs even among infants less than 4000g because of the body habitus changes in these fetuses described above. • For these reasons, as well as the inherent difficulty in predicting fetal weight, the optimal estimated weight threshold for elective cesarean delivery in diabetic gravida is controversial. Next Slide
As you can see Jaquita’s risk for shoulder dystocia is much higher since she has gestational diabetes. Return to Previous Slide
RISK FACTORS • Previous shoulder dystocia: • One database of 37,465 vaginal deliveries in Louisiana found 2 percent were complicated by shoulder dystocia. • Of the women in that 2 percent that had a second vaginal delivery…14 percent of them had a recurrent dystocia. • 5 of these 17 infants suffered birth trauma (3 permanent injuries and 1 death). Next Slide
RISK FACTORS • Postterm pregnancy: • A large proportion of deliveries complicated by shoulder dystocia occur in postterm pregnancies, although the majority of postterm pregnancies are not complicated by shoulder dystocia. • As an example, a cohort study of term (n=379,445) and postterm (n=65,796) births from Norway reported a relative risk (RR) of 1.3 for shoulder dystocia in the postterm group. • Fetal size was primarily responsible for the increased risk of shoulder dystocia after stratification by birth weight. Next Slide
RISK FACTORS • Male fetal gender: • The frequency of male gender is higher in pregnancies complicated by shoulder dystocia cases (55 to 68 percent) than in the overall birth population (51 percent). • This is the result, in part, of the relationship between fetal macrosomia and gender. This was illustrated in a study that found that 70 percent of newborns weighing >4545 grams (10 pounds) were male. • However, anthropomorphic dimensions may also account for some of the increased risk of shoulder dystocia in males. Next Slide
RISK FACTORS • Advanced maternal age: • Advanced maternal age has been identified as a risk factor for shoulder dystocia; however, confounding variables such as gestational diabetes and maternal weight probably account for this association. • This conclusion is supported by a large population series (n=75,979) which did not find maternal age affected the incidence of shoulder dystocia after correction for other risk factors. Next Slide
RISK FACTORS Summary • Maternal diabetes and macrosomia are the strongest independent risk factors for shoulder dystocia. • The highest risk of shoulder dystocia occurs when these risk factors occur together due to the combined effects of the unfavorable anthropomorphic dimensions of the IDM and large absolute size (show table 2). • However, at least 50 percent of pregnancies complicated by shoulder dystocia have no risk factors; thus, the predictive value of any one or combination of risk factors for shoulder dystocia is low. Next Slide
As shown before, when maternal diabetes and fetal macrosomia mix…shoulders get stuck. Return to Previous Slide
Vignette • Since she is post-term and nothing good happens after 41 weeks…you decide to induce Jaquita. • Labor has been fine, she has progressed like she should, and is now complete and ready to push. • You gown up and are ready to catch this baby. • The head begins to come out and…Oh crap…..Turtle Sign. • Click HERE for a purely representative and graphical demonstration.
Turtle Sign Demonstration Oh crap, Turtle Sign! Replay Demonstration Next Slide
Vignette • So you think to yourself “Dang, I should not have drank so much during my ALSO course.” • What is that Mnemonic to help you remember what to do? Next Slide
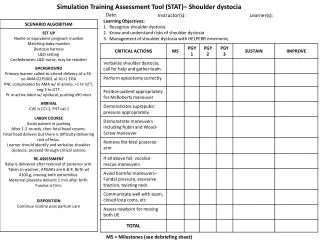
HELPERR Mnemonic • The HELPERR mnemonic is a clinical tool that offers a structured framework for coping with shoulder dystocia. • These maneuvers are designed to do one of three things: • Increase the functional size of the bony pelvis through flattening of the lumbar lordosis and cephalad rotation of the symphysis (i.e., the McRoberts maneuver) • Decrease the bisacromial diameter, the breadth of the shoulders, of the fetus through application of suprapubic pressure. • Change the relationship of the bisacromial diameter within the bony pelvis through internal rotation maneuvers. Next Slide
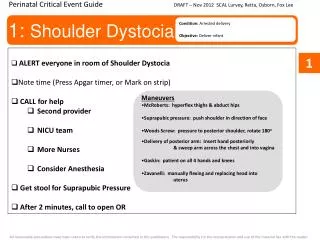
HELPERR Mnemonic • H Call for Help: • This refers to activating the pre-arranged protocol or requesting the appropriate personnel to respond with necessary equipment to the labor and delivery unit. • Click HERE for Diagram. Next Slide
HELPERR Mnemonic • H Call for Help: • This refers to activating the pre-arranged protocol or requesting the appropriate personnel to respond with necessary equipment to the labor and delivery unit. • Click HERE for Diagram. Click Diagram to Dismiss it
HELPERR Mnemonic • E Evaluate for episiotomy: • Episiotomy should be considered throughout the management of shoulder dystocia but is necessary only to make more room if rotation maneuvers are required. Shoulder dystocia is a bony impaction, so episiotomy alone will not release the shoulder. • Because most cases of shoulder dystocia can be relieved with the McRoberts maneuver and suprapubic pressure, many women can be spared a surgical incision. Next Slide
HELPERR Mnemonic • L Legs (the McRoberts maneuver): • This procedure involves flexing and abducting the maternal hips, positioning the maternal thighs up onto the maternal abdomen. This position flattens the sacral promontory and results in cephalad rotation of the pubic symphysis. Nurses and family members present at the delivery can provide assistance for this maneuver. • Click HERE for McRobert’s Diagram. Next Slide
McRobert’s Maneuver Click Diagram to Dismiss it
HELPERR Mnemonic • P Pressure (Suprapubic): • The hand of an assistant should be placed suprapubically over the fetal anterior shoulder, applying pressure in a cardiopulmonary resuscitation style with a downward and lateral motion on the posterior aspect of the fetal shoulder. This maneuver should be attempted while continuing downward traction. • Click HERE for Diagram. Next Slide
Suprapubic Pressure Click Diagram to Dismiss it
HELPERR Mnemonic • E Enter maneuvers (internal rotation): • These maneuvers attempt to manipulate the fetus to rotate the anterior shoulder into an oblique plane and under the maternal symphysis. Next Slide
"Enter" Maneuvers 1. 2. 3. • 1. Rubin II At vaginal examination apply pressure as indicated. If shoulders move into the oblique diameter, attempt delivery. • 2. Rubin II + Woods corkscrew maneuverIf unsuccessful, add the Woods corkscrew maneuver and continue rotation in the same direction. Use both hands and apply pressure as indicated. If shoulders now move into the oblique, attempt delivery. If this is unsuccessful, continue rotation 180 degrees and deliver. • 3. Reverse Woods corkscrew maneuverIf the last maneuver is unsuccessful, change to reverse Woods corkscrew maneuver. Slide fingers down to back of posterior shoulder and attempt 180-degree rotation in the opposite direction. Next Slide
HELPERR Mnemonic • R Remove the posterior arm: • Removing the posterior arm from the birth canal also shortens the bisacromial diameter, allowing the fetus to drop into the sacral hollow, freeing the impaction. • The elbow then should be flexed and the forearm delivered in a sweeping motion over the fetal anterior chest wall. • Grasping and pulling directly on the fetal arm may fracture the humerus. • Click HERE for Diagram. Next Slide
Removing Posterior Arm • R Remove the posterior arm: • Removing the posterior arm from the birth canal also shortens the bisacromial diameter, allowing the fetus to drop into the sacral hollow, freeing the impaction. • The elbow then should be flexed and the forearm delivered in a sweeping motion over the fetal anterior chest wall. • Grasping and pulling directly on the fetal arm may fracture the humerus. • Click HERE for Diagram. Click Diagram to Dismiss it
HELPERR Mnemonic • R Roll the patient: • The patient rolls from her existing position to the all-fours position. • Often, the shoulder will dislodge during the act of turning, so that this movement alone may be sufficient to dislodge the impaction. • In addition, once the position change is completed, gravitational forces may aid in the disimpaction of the fetal shoulders. • Click HERE for Diagram. Next Slide
HELPERR Mnemonic • R Roll the patient: • The patient rolls from her existing position to the all-fours position. • Often, the shoulder will dislodge during the act of turning, so that this movement alone may be sufficient to dislodge the impaction. • In addition, once the position change is completed, gravitational forces may aid in the disimpaction of the fetal shoulders. Click Diagram to Dismiss it
Vignette • So, you go to work armed with your HELPERR mnemonic. • You try everything and since you are an amazing Doctor, the baby is delivered without complications. • Although, Jaquita and Jaquita Jr. had no complications, can you name some of the complications of shoulder dystocia? • Click HERE for answers.
Complications of Shoulder Dystocia • Maternal • Postpartum hemorrhage • Rectovaginal fistula • Symphyseal separation or diathesis, with or without transient femoral neuropathy • Third- or fourth-degree episiotomy or tear • Uterine rupture • Fetal • Brachial plexus palsy • Clavicle fracture • Fetal death • Fetal hypoxia, with or without permanent neurologic damage • Fracture of the humerus Next Slide
Vignette • How do we prevent shoulder dystocia? • So should we induce or do elective C-Sections in women with Dystocia risk factors? • Click HERE for Discussion.
Prevention • Evidence is lacking to support labor induction or elective cesarean delivery in women without diabetes who are at term when a fetus is suspected of having macrosomia. • In two studies of 313 women without diabetes, induction for suspected fetal macrosomia did not lower the rates of shoulder dystocia or cesarean delivery, nor did it improve the rates of maternal or neonatal morbidity. • While labor induction in women with gestational diabetes who require insulin may reduce the risk of macrosomia and shoulder dystocia, the risk of maternal or neonatal injury is not modified. • Not enough evidence is available to routinely support elective delivery in this population. Next Slide
Prevention • So, prophylactic cesarean delivery is not recommended as a means of preventing morbidity in pregnancies in which fetal macrosomia is suspected. • Analytic decision models have estimated that 2,345 cesarean deliveries, at a cost of nearly $5 million annually, would be needed to prevent one permanent brachial plexus injury in a patient without diabetes who had a fetus suspected of weighing more than 4,000 g. Next Slide
Prevention • One method of preliminary intervention for shoulder dystocia in a patient with risk factors involves implementing the "head and shoulder maneuver" to "deliver through" until the anterior shoulder is visible. • This step is accomplished by continuing the momentum of the fetal head delivery until the shoulder is visible. • After controlled delivery of the head, the physician proceeds with immediate delivery of the anterior shoulder without stopping to suction the oropharynx. Next Slide
THE END • Good job you saved Jaquita and little Jaquita Jr. • You’re the best Doctor ever!
References • Jazayeri, A. MD, PhD & Contreras, D. MD. Macrosomia. Retrieved March 12, 2006 from web site: http://www.emedicine.com/med/topic3279.htm • Forouzan, I. MD & Mabel M Bonilla, MD. Dystocia. Retrieved March 12, 2006 from web site: http://www.emedicine.com/med/topic3280.htm • Baxley, E. M.D & Gobbo, R. M.D. Shoulder Dystocia. American Family Physician, Vol. 69/No. 7 (April 1, 2004). Retrieved March 12, 2006 from http://www.aafp.org/afp/20040401/1707.html • Rodis, J MD. Management of fetal Macrosomia and Shoulder Dystocia. Retrieved March 12, 2006 from http://www.utdol.com/utd/content/topic.do?topicKey=labordel/6688&type=A&selectedTitle=1~11