Download
1 / 47
470 likes | 649 Vues
Sexual assault in children. Dr Helen Hammond Consultant Paediatrician RCOG Stirling May 2010. “It’s everyone’s job to make sure I’m alright”. Every child matters. content. definition of a child, when is a child not a child? w hat do we mean by adolescence? what makes them different?

E N D
Sexual assault in children Dr Helen Hammond Consultant Paediatrician RCOG Stirling May 2010 “It’s everyone’s job to make sure I’m alright” Every child matters
content • definition of a child, when is a child not a child? what do we mean by adolescence? • what makes them different? • what do we know about the ways children and adolescents present to sexual abuse services? • consent and confidentiality? • what does that tell us about service design?
Definition from working together 2006 • ‘Sexual abuse involves forcing or enticing a child or young person to take part in sexual activities, including prostitution, whether or not the child is aware of what is happening. The activities may involve physical contact, including penetrative (including rape, buggery or oral sex) or non-penetrative acts. They may include non-contact activities such as involving children in looking at, or in the production of on-line images, watching sexual activities or encouraging children to behave in sexually inappropriate ways’
Definition of a child • ‘Boy or girl between birth and physical maturity’ Chambers Encyclopedic English Dictionary • … lacking experience or understanding… • legal definitions eg Children’s Act, sexual offences legislation- under 16 years/ 18 years • gradual transition childhood adulthood • frequently mismatch between physical and emotional maturity
Definition of an adolescent?? • from the Latin adolescere to grow up • stage of development between child and adult usually between 13 and 16yrs • physical and emotional changes as a result of hormonal activity
13 or thirty? • appearances very deceptive! piercings etc • language suggestive of much greater understanding…. • some young people very mature in their thinking • every one an individual….
What do we mean by child protection? • has suffered, at risk of suffering significant harm • sexual , physical, emotional harm • different pattern from adult presentations • chronic/historical rather than acute • multiple abuse • same rigor to gather evidence
Forms of sexual abuse of boys and girls • Non-contact - Exhibitionism: exposure of genitalia, sexual acts in front of child - Involving child in pornography - Sexually explicit/erotic talk • Contact - Fondling or oral contact - Masturbation: abuser/child, child/abuser - Insertion fingers or objects in anus or vulva - Penile penetration (or attempted) vagina or anus
child protection? • sexual abuse/offences very hard to prove • adult’s word against child’s • but child’s statement most powerful evidence • proportion where positive physical signs tiny even where direct contact • remarkable healing processes
adolescence… • illness/condition behaves differently • eg diabetes • physical signs of csa through puberty • young person responds differently • developing a sense of identity, what they want from life, experimentation • emerging sexuality approach needs to be different
Childhood and Adolescence… • British Paediatric Association….’a child is not simply a small adult’ • RCPCH….championing specific needs of adolescence e-Learning programme launched July 2008 • Diploma in forensic and clinical aspects of sexual assault: identifies adolescents as specific group
How children/young people present: • disclosure/allegation • ano-genital symptomatology bleeding, pain, discharge, pregnant, seeking contraception • physical symptoms eg abdominal pain • behavioural: acting out, difficult, sexualised • behavioural: withdrawn, low self esteem, eating disorder
Profile of youngsters seen • most vulnerable ‘looked after’, YPCs,, ‘alternative curriculum,’ runaways, prostitution • alcohol and substance misuse • mental health problems: self harm, eating disorders • risk taking behaviours
Profile of youngsters seen • physical and/or learning difficulties • previously abused • low self esteem • frequently repeated presentations
Signs in child sexual abuse • percentage of children reporting genital abuse in whom there are abnormal findings only 4-5% Berenson 2000, Heger 2002. • healing patterns in ano-genital injuries Heppenstall- Heger 2003- usually no residua • Adams 2005 revision Approach to the Interpretation of Medical and Laboratory findings in Suspected Child Sexual Abuse: few findings diagnostic of sexual contact • RCPCH csa guidance 2008- under revision
Sexually transmitted infections in adolescent girls • at particular risk of contracting STDs • Gonorrhoea (0.61%) and Chlamydia (3.4%) highest in 14-19 girls compared to any other sex or age group • especially vulnerable to HIV • mixture of physiological (cervical histology, contraceptives, pregnancy) and psycho-social factors • higher risk of developing pelvic inflammatory disease • Tarr and Gilliam, Chicago Clin Obstet Gynaecol 2008
Referral from paediatricians to GUM (JPFs) • Dr C Thompson reviewed 3 year period 2003-5 • 90 referrals 10 boys, 80 girls • 1-15 yrs mean 13 yrs • 60 historic or recent abuse • 1 genital warts • 2 chlamydia • 30 symptomatic no history of abuse • 1 genital herpes • 5 genital warts
Under age sexual activity: When should we be concerned? • young children straightforward- ‘duty to protect’ • young people deemed competent seem straightforward… • young people where we doubt competence more difficult… • eg infatuated 15 yr olds, vulnerable groups
Confidentiality • GMC Guidance (0-18 yrs guidance for all doctors, October 2007) new guidance coming… • RCPCH guidance 2004 • CMO guidance • new legislation….
Confidentiality – GMC 2000 Para 36:disclosure without consent where failure to do may expose the patient to risk of death or serious harm Para 37:disclosure to assist in the detection, prevention, or prosecution of a serious crime Para 39:disclosure if doctor believes the patient to be victim of neglect or physical, sexual or emotional abuse and the patient cannot give or withhold consent..in the patient’s best interests…
When to breach confidentiality • RCPCH guidance February 2004‘Responsibilities of doctors in child protection cases with regard to confidentiality’ www.rcpch.ac.uk • the doctor’s primary duty is to act in the child’s best interests. If there is a conflict of interests between doctor and parents or parents and child, then the child’s needs are paramount.
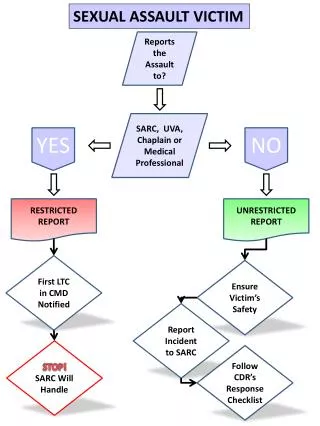
REFERRAL FOR UNDER- AGE SEXUAL ACTIVITY INFORMATION SHARING & RISK ASSESSMENT NO EVIDENCE ABUSE EXPLOITATION BUT RECOGNISING RISK FACTORS E.G LAC / SUBSTANCE MISUSE EVIDENCE OF ABUSE/EXPLOITATION NO EVIDENCE OF ABUSE /EXPLOITATION CP INTERAGENCY PROCEDURE Health route MULTIAGENCY ASSESSMENT New Concern IRD CCH/ GP SERVICES SEXUAL HEALTH SERVICES FAMILY PLANNING CLINIC GENITO URINARY MEDICINE New Concern MULTI AGENCY SUPPORT PLAN JOINT POLICE/ SW INTERVIEW JOINT PAED/FORENSIC EXAMINATION REVIEW, ADVICE , HEALTH PROMOTION , EDUCATION CHILD PROTECTION PLAN INCLUDING HEALTH PLAN
Scottish govt guidance:under age sexual activity • Long gestation… • New legislation • Building on good practice
Risk assessment ‘tool’ • age differential • any imbalance of power • overt aggression • evidence of coercion or bribery • substances used as a disinhibitor • has young person’s own behaviour placed them at risk e.g. under influence of alcohol/drugs
Risk assessment ‘tool’ • is the young person able to give informed consent e.g. learning disability, mental illness • have unusual attempts been made to keep relationship secret • does the young person accept, deny or minimise concerns • is there evidence of grooming
Initial Referral Discussion Police Social Work Referrer Health • Share relevant information • Plan investigation: interview, medical, etc • Agree sequence, timing, venue, people, consent
Paediatric forensic examination • combines the need for medical evaluation and evidence gathering into one examination • skills, competencies and facilities required set out in joint RCPCH/ AFP (Association of forensic Physiciansguidance 2004, 2007)
RCPCH/Faculty of forensic and legal medicine • single examiner if both sets of skills…?corroboration • use of colposcope to allow photo-documentation essential in paediatric examinations • access to peer review/second opinion
Consent • Informed consent (written) must be sought from the parent/carer or young person to: • Comprehensive and sensitive examination • Forensic sampling • Photo-documentation • Information sharing, Report writing • Use of images in teaching/training and peer review Age of legal capacity (Scotland) Act 1991
approach to the examination of older children/adolescents • describe the process in detail • give a sense of control • choose the right support person • keep talking- and smile! • discuss the findings and what will happen next… • ask permission to discuss the findings with others (including parent)
Interpretation of the findings • knowledge of pre- and post pubertal genital appearances • knowledge of the morphological changes during puberty • knowledge of the appearances following healing of injuries partic across puberty
Pitfalls and dilemmas… • is it a normal variant? • when is bleeding a sign of abuse? Possible differential diagnoseseg lichen sclerosis atrophica, puberty • could it be trauma? Straddle injury, toilet seat! • when is infection a sign of abuse? possible differential diagnoses recurrent vulvo-vaginitis, warts.
Process of examination in sexual abuse/assault • behaviour,demeanour, emotional state • state of clothing, piercings etc • growth • maturity/pubertal stage (thelarch, menarch…) • superficial injuries - head and neck, mouth, breasts, arms, inner thighs, buttocks, perineum, genitalia, anus • detailed exam using colposcope
Process of examination • forensic sampling • screening for sexually-transmitted infections • post-exposure prophylaxis – HBV/HIV • post-coital contraception • therapeutic support and counselling
Young people’s experience of sexual abuse examinations O’Donnell and Hammond 2009 prelim findings • ‘Feeling nervous…finding it scary’ • didn’t like the doctor- ‘she didn’t smile’ • ‘Difficult and upsetting’- didn’t feel she could have asked the doctor to stop • would have liked more explanation of what was going to happen and what was found.
Long term sequelae • risk taking behaviours • teenage pregnancy • mental health problems • relationship difficulties • child protection concerns in the next generation
Challenges • delivering accessible/approachable services • confidentiality • child protection • working with parents • inter-agency working • negotiating policy and protocols • the LAW!
Models of service delivery • paediatric colposcopy facility • adult rape service • co-located unit • managed clinical network(s) • multi-disciplinary/agency ‘one stop shop’ (e.g. Sexual Assault Referral Centre)
The way forward… • many models of good practice • consistent and proportionate agency responses • need focus on prevention and health promotion • involve young people in developing the service
references • Child Protection Companion: RCPCH 2006 • Physical signs of child sexual abuse RCPCH 2008 • RCPCH/FFLM Paediatric forensic examinations in relation to csa RCPCH 2007 • Adams JA Approach to the Interpretation of Medical and Laboratory findings in Suspected Child Sexual Abuse 2005 revision • Tarr ME and Gilliam ML Clin Obstet & Gynaecol Vol 51, No 2 306-318 2008