Download
1 / 81
880 likes | 1.39k Vues
Clostridium Difficile Associated Diseases. 陈佰义 , M.D . PhD Division of Infectious Diseases Infection Prevention and Control Team The First Hospital of China Medical University May 2010. AAD antibiotic-associated diarrhea. CDAD. hospital-acquired diarrhea. 2.

E N D
Clostridium Difficile Associated Diseases 陈佰义, M.D. PhD Division of Infectious Diseases Infection Prevention and Control Team The First Hospital of China Medical University May 2010
AAD antibiotic-associated diarrhea CDAD hospital-acquired diarrhea 2
Antibiotic Associated Diarrhea? infectious • Most causes unknown. • Several candidates studied • Clostridium difficile is the major recognized cause • Candida species • Clostridium perfringens • Staphylococcus aureus • Serendipitous infection by viruses, Salmonella, etc. • Non-infectious changes in colonic fatty acid and carbohydrate metabolism induced by antibiotics
C difficile-causative agent in: 10-25 % of patients with AAD 50-75 % of patients with antibiotic-associated colitis (AAC) 90-100 % of patients with PMC Aslam et al, Lancet Inf. Dis, 2005 AAD antibiotic-associated diarrhea CDAD hospital-acquired diarrhea 4
Confusing terminology • Antibiotic-associated diarrhea(AAD) • C. difficile is only one cause • Clostridium difficile-associated diarrhea(CDAD) • diarrhea + positive stool test • Clostridium difficile colitis(CDC) • underlying pathologic process • Pseudomembranous colitis(PMC) • endoscopic demonstration of exudative lesions • Toxic megacolon • radiologic and surgical diagnosis Clostridium Difficile-Associated Disease
Clostridium Difficile Associated Diseases • History and Epidemiology • Pathogenesis • Clinical pictures • Diagnosis • Management • Prevention and control • Future • Summary
History • 1893-first case of PMC -reported as diphtheritic colitis. • 1935-“Bacillus difficile” first isolated -Hall & O’Toole • 1970s-antibiotic-asociated colitis identified. • 1977 - Birmingham General Hospital-C. difficileidentified as cause • 1978-C. difficile toxins identified in humans. • 1979-therapy with metronidazole or vancomycin • 2000-increased incidence and virulence microbiology • The “difficult clostridium” • Obligate anaerobe/Motile • G+ spore–formomg bacillus • spores resistant to Heat/Desiccation/Disinfection/Alcohol • Source • Environment • Stool flora
Why are we concerned? Increasing numbers of infections. Potential for severe disease Emergence of hypervirulentstrainsthat may be more transmissible and/or cause more severe disease e.g. ribotype O27. Concerns over possible antibiotic resistance. Increasingly recognized as a major nosocomial pathogen capable of causing outbreaks 8
Increase in cases More than 50,000 cases reported in England in 2007 Fifty-fold increase since 1990; 20% of cases <65 9
National Estimates of US Short-Stay Hospital Discharges with C. difficile as First-Listed or Any Diagnosis 10 From McDonald LC, et al. Emerg Infect Dis. 2006;12(3):409-15
C.difficile deaths CDAD cited on 1 in every 250 death certificates in 2005 Further 72% increase in 2006 11
CDAD Rates and Mortality Increasein Parallel with Patient Age Loo et al NEJM 2005;353:2442-9
Acute care hospitals with CDADoutbreaks between 2001 and 2004
Clostridium Difficile Associated Diseases • History and Epidemiology • Pathogenesis • Clinical pictures • Diagnosis • Management • Prevention and control • Future • Summary
CDAD • Transmission: • Carried in GIT of 3% of general population • Up to 30% of hospitalized patients become colonized • Fecal-Oral Route -sensitive individuals can become infected if they touch items or surfaces that are contaminated with feces and then touch their mouth or mucous membranes. • Hands of hospital personnel are important intermediary -can spread the bacteria to other patients or contaminate surfaces with contact.
Pathogenicity of C. difficile • Exotoxin A (enterotoxin) : • MOA unknown/causes outpouring of fluid and a watery diarrhea • Exotoxin B (cytotoxin): • damages colonic mucosa leading to pseudomembrane formation • mechanism is via ADP-ribosylation of Rho (a GTP-BP) • this causes depolymerization of actin in the cytoskeleton • Pathogenicity in apathogenicity locus (PaLoc) of five genes • Binary toxin-its clinical significance is unravelling Spigaglia and Mastrantonio. J Clin Microbiol. 2002 Sep;40(9):3470-3475.
Host Protection AgainstCDAD Occurs at Two Levels • Normal bacterial flora -prevent establishment of C. difficile colonization of the GI tract • Antibodies (serum and mucosal?) -prevent CDAD disease if colonization occurs -Antibodies are probably first acquired in infancy
Risk Factors Age >65 years Severe underlying disease Antimicrobial therapy Clindamycin, 3rd G cephalosporins, penicillin, FQs Nasogastric intubation Anti-ulcer medications Proton pump inhibitors Chemotherapy Long hospital stay or long-term care residency 20
Role of Antibiotics in CDAD • Any antibiotic may be associated with CDAD. • Disruption of normal intestinal flora -the determining antibiotic event • susceptibility window:following an antibiotic there is a variable-length window during which a patient is susceptible. • C. difficile resistance to the precipitating antibioticis thought to be important, but is not always present (e.g. ampicillin).
Time-Course of Antimicrobial Effect onthe Normal Gut Flora and CDAD Risk No Antibiotics Normal Flora Antibiotic Use Flora Disrupted No Antibiotics Flora Disrupted No Antibiotics Normal Flora 1. C. difficile resistanceto the antibiotic used enables the organism to infect while the antibiotic is being given. 2.Resistant and Susceptible C. difficilecan infect after the antibiotic has been stopped and the flora remains disrupted. 1. 2. Variable Time No risk of CDAD Higher risk of CDAD, if C. difficile is resistant to the Abx used High risk of CDAD, C. difficile resistance is not an issue No risk of CDAD
Original (Incorrect) Hypothesis for C. difficile Hospital Infection
Rate of CDAD in Patients Colonized and Non-colonized with CD • Data from four prospective studies in which rectal swab cultures were obtained weekly from hospitalized patients *Risk difference: –2.34%; 95% CI: -4.34, -0.34%; P= 0.021 • The risk was also significantly decreased when only patients who received antibiotics were analyzed. (P=0.024) Shim JK, et al. Lancet 1998;351:633-636
Revised Hypothesis for CDAD Acquisition of a toxigenic strain of C. difficile and failure to mount an anamnestic Toxin A antibody response results in CDAD.
Pathogenesis of CDAD Owens, CID, 2008, 46, S19-31 26
Pathogenesis of CDAD 27 Poutanen, S. M. et al. CMAJ 2004;171:51-58
TcdC Variants Challenges -Emergence of a new outbreak epidemic strain in U.S. Quebec and Europe • 18 bp deletion in tcdCgene of PaLoc • Could lead to increased toxin production (18-fold fortoxin A, 23-fold for toxin B) observed by Warny et al.2 • Highly resistant to FQs and clindamycin • Metronidazole, vancomycin susceptible
Epidemic C. difficile Strains ProduceIncreased Toxins A and B in vitro • Epidemic strains from Quebec/UK/US-carry binary toxin/have tcdC deletion/toxinotype III tested in vitro for toxin A and B,(compared with non-epidemic toxinotype 0 strains). NAP1 / ribotype 027 log phase stationary phase • Toxin A/B 16-23 fold higher in toxinotype III isolates (P<.0001). • Toxinotype III isolates produce toxins during the log phase whereas toxinotype 0 strains did not produce toxin until the stationary phase Warny, et al. Lancet 2005;366:1079-84
Epidemic C. difficile Strains ProduceIncreased Toxins A and B in vitro NAP1 / ribotype 027 log phase stationary phase Warny, et al. Lancet 2005;366:1079-84
States with the epidemic strain of C. difficile confirmed by CDC 11/15/2005 (N=16)
States with the Epidemic Strain of C. difficile Confirmed by CDC and Hines VA labs (N=23),Updated 2/9/2007 DC HI PR AK
Outbreak Strains are NOT New: Comparisonof Historic and Epidemic REA “BI” types • Historic BI (Bee-Eye) isolates were found from 1983 to 1992, were of BI types BI1 to BI5, contained binary toxin genes, and the 18 bp deletion in the tcdC gene. • Historic isolates were NOT resistant to newer fluoroquinolone antibiotics. • New epidemic BI isolates (types BI6-BI19) are uniformly resistant to the newer FQs (gatifloxacin, moxifloxacin).
Is Increased Toxin A and B in vitro the Answer to Increased Pathogenicity? Previous measures of toxin A and B production in vitro have not correlated with disease severity in hamsters. Preliminary data from hamster studies with REA type BI isolates show mortality rates similar to high virulence controls. Borriello et al J Med Micro 1987;24:53-64
What is the Role ofFluoroquinolone Resistance? • Resistance to newer fluoroquinolones (gatifloxacin and moxifloxacin) is the only detectable difference between historic nonepidemic BI group isolates and epidemic current BI group isolates. • Fluoroquinolone use has been a risk factor for CDAD in hospitals with outbreaks caused by the epidemic strain of C. difficile. Gaynes et al CID 2004;38:640-645; Pepin et al CID 2005;41:(1) ;Loo et al NEJM 2005;353:2442-2449
Clostridium Difficile Associated Diseases • History and Epidemiology • Pathogenesis • Clinical pictures • Diagnosis • Management • Prevention and control • Future • Summary
Clinical Presentation Asymptomatic colonization Mild disease Non-bloody diarrhea Mild abdominal tenderness Severe disease Pseudomembranous colitis Paralytic ileus Ileitis Toxic megacolon Ulcerative colitis Perforation(peritonitis) Ascites 37
Clinical presentation: Epidemic Similar to old cases but more severe More toxic megacolon (less diarrhea) Profound leukemoid reactions Severe hypoalbuminemia (PLE) Septic shock Need for colectomy Increased mortality Ann Intern Med 2006;245
Leukocytosis and CDAD – Do Not Missthis Clue to Possible Fulminant Disease • Toxin A is a potent neutrophil chemoattractant • CDAD found in 16% of patients with WBC>15,000/mm3 25% of patients with WBC>30,000/mm3. Clin Infect Dis 2002;34:1585-92 • 58% of 60 patients with unexplained WBC >15,000/mm3 had CD toxin in stool. AJM 2003;115:543-6
Clostridium Difficile Associated Diseases • History and Epidemiology • Pathogenesis • Clinical pictures • Diagnosis • Management • Prevention and control • Future • Summary
Diagnosis of CDAD • S/S • Endoscopy (pseudomembranous colitis) • Culture • Cell culture cytotoxin test • EIA toxin test • PCR toxin gene detection
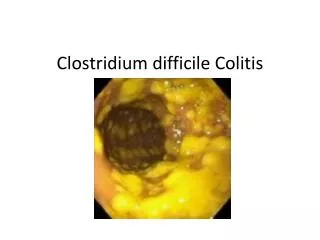
Pseudomembranous Colitis Yellow lesion against hyperemic bowel Mushroom-shaped pseudomembrane→ “Volcano” lesion 45 H & E, OM 400x
Laboratory diagnosis Culture Easy and sensitive but slow High carriage rates in hospitalised patients Non-toxigenic isolates detected as well Not used for initial diagnosis now Toxin detection in faeces Cell culture “Gold standard” but relatively slow Enzyme immunoassays(EIA) Rapid/cheap/specific Need test to include Toxin A and B Variable sensitivity Asymptomatic carriage issue Single negative result does not exclude infection Regardless of method you must take clinical picture into account! 46
CDAD Case Definition Stool characteristic Diarrhea (most common) No diarrhea Associated with toxic megacolon or ileitis Documented by radiology ≥ 1 of the following Stool positive for: C. difficile toxin C. difficile determined to be a toxin producer Pseudomembranous colitis by: Endoscopy Histological exam 48
Clostridium Difficile Associated Diseases • History and Epidemiology • Pathogenesis • Clinical pictures • Diagnosis • Management • Prevention and control • Future • Summary