Download
1 / 12
270 likes | 1.49k Vues
Chronic Inflammatory Demyelinating Polyneuropathy. By : Kyle Leato, SPTA. OBJECTIVES. Provide background information Clinical Presentation Cause Treatment Importance to Physical Therapy Conclusion. Background Information. What is CIDP?

E N D
Chronic Inflammatory Demyelinating Polyneuropathy By: Kyle Leato, SPTA
OBJECTIVES • Provide background information • Clinical Presentation • Cause • Treatment • Importance to Physical Therapy • Conclusion
Background Information • What is CIDP? • It is a common, under diagnosed immune-mediated inflammatory disorder of the peripheral nervous system. (Hartung, et al., 2005) • Commonly referred to as: • chronic relapsing polyneuropathy • Closely related to: • Guillain-Barré syndrome. • Prevalence: • 0.5 out of 100,000 children • 1-2 per 100,000 adults
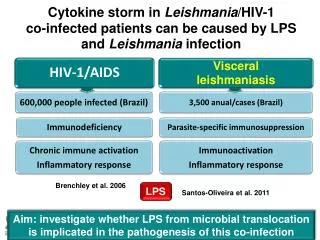
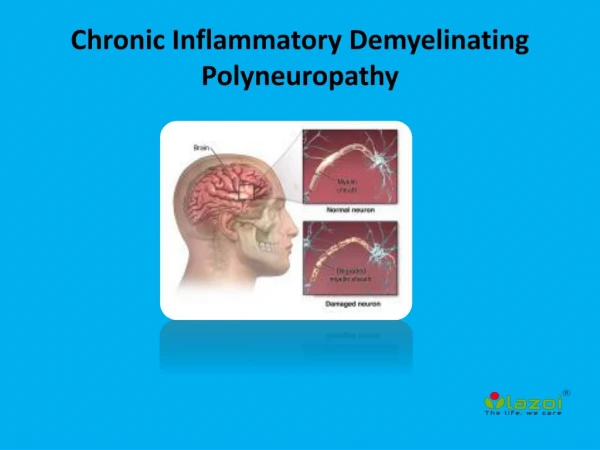
Cause • The body’s immune system attacks the nerves in the periphery, affecting the limbs and organs of the body (Forsberg, Press & Westblad, 2009)
Symptoms • Occurrence of symmetrical weakness in both proximal and distal muscles that progressively increases for more than 2 months. • Impaired sensation, burning and weakness ( generally occurring in the feet first and they gradually ascend to involve other parts of the body). • Absent or diminished tendon reflexes. • Elevated CSF protein level. • Signs of demyelination (in nerve biopsy specimens). • Foot drop. • When organs become involved: inability to adequately empty the bladder, nausea, vomiting, abdominal fullness or bloating, diarrhea, or constipation, low blood with dizziness, or trouble maintaining an erection. ****The severity and the combination of symptoms vary for each patient.
Treatment • Early Stages: • Typically PROM and positioning is used. • Family Education • Middle Stages: • Tactile re-training (brushing, vibration and tapping) • Light resistive exercises • PNF if the patient is capable • Late Stages: • Transfer Training • Gait Training with the use of an AD • Progressive Resistive Exercises
Other Treatment Ideas • Land Based Exercising: • Alter G Treadmill for reduced body weight walking. Increased weight bearing over a period of time is shown to increase strength and the ability to ambulate independently. (Greenwood & Tuckey, 2004) • Water Based Exercise: • Hydro Physio Underwater Treadmill can be altered by increasing or decreasing the amount of water in the tank. • Aquatic therapy has shown to be very beneficial to one of our own patients.
Youtube Video https://www.youtube.com/watch?v=6Y1glEYQAJs
Importance in Relation to Physical Therapy • What can we as a physical therapy team do? • Be prepared to treat the patient on a day-to-day basis because every day can be a day of progression and/or setbacks. Be ready for anything. • Interdisciplinary communication between medical team, occupational therapy and speech therapy. • We can provide education for the patients and their support systems. • Maintain a positive attitude and optimistic outlook. • MOVEMENT IS THE BEST MEDICINE!
Conclusion • It’s important to know that CIDP is a unique diagnosis to each and every patient. (Barohn, et al., 2010) • No treatment will be the same, therefore it is important to be aware of their past history, their past and current symptoms, as well as their current lifestyle. • There is no specific “cure” that physical therapy can provide, so we make it a goal to use the techniques, exercises and knowledge that we have in order to best improve the quality of the life of the patient.
References • Barohn, et al. Chronic Inflammatory Demylinating Polyneuropathy Disease Activity Status: Recommendations for Clinical Research Standards and Use In Clinical Practice. Journal of the Peripheral Nervous System. 2010; 15(4): 326-333. • Forsberg A, Press R, Westblad ME. Disability and health status in patients with chronic infammatory demyelinating polyneuropathy. Disability & Rehabilitation. 2009; 31(9): 720-725. • Greenwood R , Tuckey J. Rehabilitation after severe Guillain-Barré syndrome: the use of partial body weight support. Physiotherapy Research International. 2004; 9(2): 96-103. • HartungH, JanderS, Kieseier BC, Köller H. Chronic inflammatory demyelinating polyneuropathy. N Engl J Med. 2005; 352: 1343-1356.