Download
1 / 37
411 likes | 1.3k Vues
Spondylolysis and Spondylolisthesis. Spondylolysis is a stress fracture of the pars interarticularis Spondylolisthesis is the forward slippage of the vertebral body away from the posterior elements. Scotty Dog Fracture. Spondylolisthesis. Wiltse Classification of Spondylolisthesis.

E N D
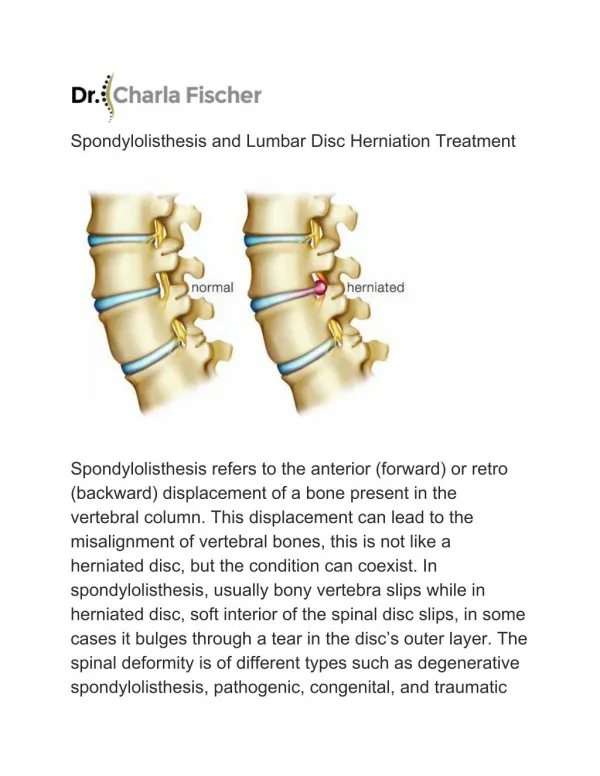
Spondylolysis and Spondylolisthesis • Spondylolysis is a stress fracture of the pars interarticularis • Spondylolisthesis is the forward slippage of the vertebral body away from the posterior elements
Spondylolysis and Spondylolisthesis • More common in Males 2:1 (except dysplastic type). However females are more likely to have progression of a listhesis. • Prevalence • Age 7 - 10: 4% • Adults: 6%
Spondylolysis and Spondylolisthesis • Meyerding’s Spondylolisthesis Grades • I. <25% slippage • II. 25 - 50% slippage • III. 50 - 75% slippage • IV. 75 - 100% slippage • V. > 100% (spondyloptosis)
Spondylolysis and Spondylolisthesis • Slip Angle • Determines amount of lumbosacral kyphosis • Measured angle of L5 inferior border and the perpendicular of posterior border of sacrum • Normal = 0 - 10 • If > 50%, is at risk for progression of listhesis
Spondylolysis and Spondylolisthesis • Sacral Inclination Angle • Measures amount of lumbosacral kyphosis • Angle of posterior aspect of sacrum and true horizontal line • Increased angle (vertical sacrum) is associated with progression of listhesis
Isthmic Type • Most common • Defect in the pars interarticularis • Genetic Role (30 - 70% familial incidence) • 15% incidence of listhesis in relatives • 50% prevalence in some eskimo tribes • spondylolysis --> repetitive stress --> gradual healing --> elongated pars
Dysplastic • Congenital (more common in females 2:1) • More genetic than isthmic (33% incidence of listhesis in relatives) • Abnormalities of upper sacrum or posterior arch of L5 • Decreased development of superior facets of sacrum • Dysplastic changes in upper sacrum, increased slip angle, hyperlordosis
Risk Factors for spondylolysis • Repetitive stress (microtrauma) • Lumbar hyperlordosis • Gymnastics, football, wrestling • Disease: myelodysplasia, cerebral palsy, spina bifida • Anterior Abdominal weight • Ambulation (listhesis only in ambulating humans)
Risk Factors for Listhesis Progression • Young age (progression is rare after 20 yo) • Female • Ligamentous laxicity • > 50% slippage • > 55% slip angle • L5 - S1 instability • Trapeaoidal L5 • Dome- shaped upper sacrum • Less likely to progress with decreased disk space and an Anterior sacral lip
Clinical Findings • Usually asymptomatic in children and is an incidental finding on x-ray. • Symptoms occur usually with pre-adolescent growth spurt • Pain localizing to low lumbar spine • increases with activity (not correlated with degree of slippage) • +/- radicular symptoms (associated with high grade slippage)
Clinical Findings • Increased lumbar lordosis • Severe listhesis: • lumbosacral kyphosis • Phalan Dickson stance (knees bent/hips flexed) • Anterior abdominal crease (ribs to iliac crest) • Hamstring tightness limited straight leg raise • Paravertebral spasm • Flat buttocks • Palpable step off • shortened torso
Clinical Findings • Lordosis above lumbosacral kyphosis • Torso shift backwards • Scoliosis • Bladder/bowel impairment • Mechanism: • nerve root irritation possibly
Imaging • A/P, lateral, Right and Left Oblique views • Scottish Terrier fracture • CT • Bone Scan - show likelihood of healing • Spectrometry - early diagnosis • Follow progression of listhesis with a lateral lumbar
Treatment • Asymptomatic (Grade I or II) • No Slippage • Participate in sports as tolerated • Not likely to progress • No lumbar loading or hyperextension
Treatment • Asymptomatic (Grade III or IV) • Posteriorlateral fusion • Especially important if skeletally immature
Treatment • Symptomatic Lysis or Grade I or II listhesis • Conservative Treatment (benign prognosis) • 80% will respond and be able to return to normal activities • Activity restriction and NSAIDS (questionable) • If pain is severe, Brace (relief up to 80% of pt.s if grade I) • Physical Therapy- Decrease extensor stresses of lumbar spine • Abdominal strenthening • Stretch paraspinals and hamstrings
Treatment • Symptomatic (grade III or IV) • Rarely respond to conservative treatment • Surgical stabilization
Treatment • Indications for Surgery • Persistant back pain which interfere with activities of daily living • Symptomatic with failed conservative treatment • Significant progression • Grade III or higher with >55 degrees slip angle • Neurologic defecits • Acute traumatic
Surgical Stabilization • Posterior interbody fusion • Fusion of L5 transverse process to sacral ala (with iliac crest graft) • Grade I or II: solid fusion and relief of symptoms 70 – 100% • Grade III or IV: Fuse L4 also • Complications: Cauda equina syndrome, progression, continued cosmetic dissatisfaction • Post – op: Pantaloon cast (prevent kyphosis) • Hamstring tightness resolves within 18 months in most cases
Surgical Stabilization Pars Defect Repair Pedicle screw fixation (healing and relief 70- 90%) Scott Wiring (up to 100% healing) Results vary Best results if lysis and not listhesis (<1-2mm slippage). Best at L1 – L4 levels. <30 year old Contraindication: Degenerative disk disease Complications: Neurologic defecits (are diminishing)
Surgical Stabilization Reduction Correction of lombosacral kyphosis Reduce compensatory lordosis above fusion Reduce stress at fusion Increase cosmetic result Success vary (25 – 30% risk of injury) Closed (pelvic suspension or hyperextension casting) Open (distraction constructs)
Surgical Stabilization Vertebrectomy With spondyloptosis L5 out, fuse L4 to S1 High risk of neurologic defecits Success varies
Surgical Stabilization Fabris et al, Spine; 1996 Combined fusion, reduction, and pedicle fixation 80% correction of deformity All had solid fusion and no complications
Treatment Summary • Spondylolysis or low grade listhesis • If conservative treatment fails, Gold standard surgery is fusion in situ. Satisfactory and lasting results • High grade slips and slip angle • Instramental fusion in situ • Combined Ant/Post fusion • Reduction and fusion • If significant neurologic defecits exists, fusion + decompression (L5 laminectomy/foramenotomy and sacroplasty) • Results are good (11/11 successful union and decompression)
References • Smith JA, Hu SS. Management of spondylolysis and spondylolisthesis in the pediatric and adolescent population. Orthop Clin North Am. 1999 Jul; 30(3): 487-49 • Garry JP, McShane J. Lumbar spondylolysis in adolescent athletes. J Fam Pract. 1998 Aug; 47(2): 145-9 • Zuckerman JD. Instructional Course Lectures 1999. Vol. 48: 532-535 • Beaty JH. Orthopaedic Knowledge Update. 1998; 699-705 • Canale TS. Operative Orthopaedics. 1998. Vol. 3 2952-2961 • Rockwood CA Fractures in Children 1996. Vol. 3: 1086-1094