Download
1 / 29
290 likes | 461 Vues
Black Bugs Blood: West Nile Virus & the Blood Supply. Infectious Transfusion Risks, Screening Blood donations for WNV and other icky things Jed Gorlin, Memorial Blood Centers Duluth TAM 11/04. Infectious Risks Viral Bacterial Protozoa Ricketsia Other ?Prion. Non-infectious risks

E N D
Black Bugs Blood:West Nile Virus & the Blood Supply Infectious Transfusion Risks, Screening Blood donations for WNV and other icky things Jed Gorlin, Memorial Blood Centers Duluth TAM 11/04
Infectious Risks Viral Bacterial Protozoa Ricketsia Other ?Prion Non-infectious risks Transfusion Reaction Metabolic Cardiac Overload Dilutional Coagulopathy TAGVHD Alloimmunization Risks of Transmission
Product Safety Donor Recruitment Donor history screening Donor Testing Manufacturing cGMP Transfusion Safety Patient blood sample Med indication for Tx. Special Tx needs Select right unit Issue to floor administration monitoring & evaluation of reaction Transfusion Safety
Paling Risk Scale for Major Transfusion Hazards 108 107 106 105 104 103 102 101 100 HIV General anesthesia HCV HBV Bacteria Mis-Transfusion TRALI TA-GVHD Cardiac Metabolic risk in neonates Under transfusion Sunny Dzik, MD
Window period risk • Why is there any residual risk? There is potential for transfusion transmission, if donors is drawn after acquiring the disease but before they make an antibody response. • Time from infectivity to test reactivity • Chance of transmission is a function of both incidence and length of window period.
NAT screening (HCV/HIV/HBV) • Two major testing platforms for HIV/HCV • Roche-Pools of 24, separate tests for HCV, HIV. Advantage: automated detection, disadvantage, very manual sample prep • Chiron-Gen Probe (TMA) Multiplex test • Pools of 16, automated sample prep, manual detection. Requires extra round to resolve positive samples. More false positives
MBC Experience • After testing almost 2,000,000 samples, MBC has detected 1 HIV NAT window period case and 5 HCV NAT+/EIA negative samples. • Almost 1,000,000 samples were tested for both HCV and HIV before a single NAT+/EIA - sample was found.
What Has NAT Testing Cost the US?? • Assume 13 million blood donations annually • Assume an average cost/donation of $16 • Cost of HCV/HIV- NAT = • $208,000,000/yr or $104M each
Cost/HCV-NAT positive donation: • Average HCV-NAT pos. rate in US = 1:276,000 donations • 13 million donations/yr collected • 47 window case donations expected @ $104,000,000 total • Cost/HCV-NAT positive donation detected = $>2,200,000/donation
Cost/HIV-NAT positive donation: • Average HIV-NAT pos. rate in US = 1:3,760,000 donations • 13 million donations/yr collected • 3.5 window case donations expected @ $104,000,000 total • Cost/HIV-NAT positive donation detected = > $28,000,000/donation
Cost-Effectiveness Comparisons Cost-effectiveness ($/YLE) 8,000,000 6,000,000 Transfusion Safety Interventions 4,000,000 2,000,000 600,000 400,000 200,000 Commonly Accepted Medical Practices RhIg/HDN HTN Annual Mammo- gram Cardiac Trans- plantation CABG (one vessel) PAD- p24 Ag Testing ALT Testing HCV Look- back SD FP Anti-HBc Testing for HIV MP NAT HIV+HCV MP=>SD NAT Prophy- CABG Therapy laxis
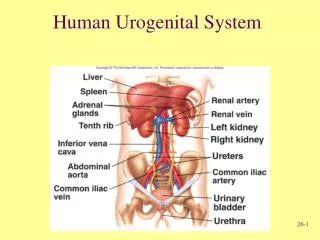
Other Transfusable Parasitic • Chagas • Trypanosoma cruzi Endemic: Central & So. America • Infected reduviid (kissing) bug falls from thatched roof, defecates and inoculates skin • May be under-recognized cause of heart failure • Only 7 cases Tx transmission in US/Canada • Screened for in Brazil and other LA countries • ARC proposes to implement screening • MBC to participate in Chagas trial ~1/05
West Nile Virus: Background and Ecology West Nile Virus: Background and Ecology • First isolated in West Nile district, Uganda, 1937 • Commonly found in humans and birds and other vertebrates in Africa, Eastern Europe, West Asia, and the Middle East, but has not previously been documented in the Western Hemisphere • Basic transmission cycle involves mosquitoes feeding on birds infected with the West Nile virus • Infected mosquitoes then transmit West Nile virus to humans and animals when taking a blood meal
The Japanese Encephalitis Serocomplexof the Family Flaviviridae
Year States Humans/ Fatalities Birds Mosquito Pools Horses 1999 4 62/6 ? 16 25 2000 11 + DC 21/2 4305 515 63 2001 27 + DC 66/9 7332 919 731 2002 44 + DC 3949/262 14,790 5938 11,450 1999 - 2002 Verified WNV Surveillance Results Reported to ArboNet
30 2001 25 2000 1999 20 Number of cases 15 10 5 0 7/7 8/4 9/1 9/29 10/27 11/24 12/23 Week ending Date of Symptom Onset, West Nile VirusUnited States, 1999-2001
Clinical Epidemiology • Incubation period 3 - 14 days • ~80% of infections are asymptomatic • 20% develop “West Nile fever” • 1 in 150 develop meningoencephalitis • Advanced age primary risk factor for severe neurological disease and death
Outcome of West Nile Virus Infection among Hospitalized Patients • At discharge (NY and NJ, 2000) • More than half did not return to functional level • Only one-third fully ambulatory • At one year (NYC 1999 patients) • Fatigue 67%, memory loss 50%, difficulty walking 49%, muscle weakness 44%, depression 38%
Summer 2003 • Implemented WNV NAT screening 7/1/03 • Automated DNA extraction • Pool size 6-dedicated pooling machines • TaqMan platform requires lots of room. Total NAT laboratory space doubled • MBC detected ~36 WNV+ blood donors, mostly in Nebraska, South Dakota and Iowa
More Automated System Hamilton Pipettor COBAS TaqMan (96/48) COBAS AmpliPrep
2004 WNV Transfusion transmission in Arizona • MMWR Sept 17, 2004 p 842 • In 2003 blood centers interdicted ~800 blood components via pooled testing. Because of 6 cases of transfusion transmission, a policy for single donor (SD) testing was implemented for 2004. • 3 days before switch to SD in Arizona (from TMA pool of 16), a 43 yo with severe diabetes was transfused following a knee amputation. He subsequently developed WNV and died. The units were traced and one donor was shown to be WNV+ by SD but not pooled testing.
Implications • Despite reduced pool size and plans to implement single donor testing, window period cases of WNV continue to occur. • There have been two HIV transmissions despite pooled NAT testing • Both manufacturers are working to create more automated systems that facilitate single donor testing. These will be more expensive, but will allow greater throughput than current manual tests