Download
1 / 13
150 likes | 171 Vues
Implementation of Community Score Card in Tanzania Experiences from Mbeya, Lindi, Mtwara and Tanga regions Presented by Erick Msoffe on behalf of MoHCDGEC. Outline. What is Community Score Card? Why Community Score Card in Health Sector Tools Methodology Results

E N D
Implementation of Community Score Card in Tanzania Experiences from Mbeya, Lindi, Mtwara and Tanga regions Presented by Erick Msoffe on behalf of MoHCDGEC
Outline • What is Community Score Card? • Why Community Score Card in Health Sector • Tools • Methodology • Results • Reactions from the Community • Key Lessons
HSSP IV Strategic Objective 3 The health and social welfare sector will achieve active community partnership through intensified interactions with the population for improvement of health and social wellbeing GIZ contribution toTGPSH include promotion and strengthening of civil society participation in health planning, implementation and monitoring
Community Score Card • It is a social accountability mechanism that brings both service providers (clinical staff, FGCs, village leadership) and users (community members) into dialogue. • The overall goal is to make unheard voices heard, increase public awareness, and by so doing, generate collective action and bottom-up influence for better service delivery
Why Community Score Card Specific objectives include;- • Ensure transparency through access to information on inputs; e.g medicines and supplies, funds, staff… • Increase accountability from demand and supply side • Improve responsiveness and quality of health service delivery through dialogue and interaction between users and providers • Allocation and reallocation of resources; focus on results or prioritizing needs (proper health planning)
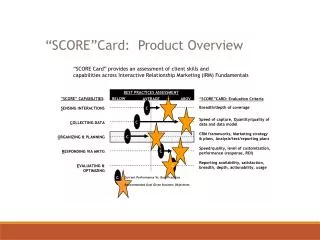
The approach The process takes two days per facility; standardised tools developed by the MoHCDGEC are used for facilitation; • Input tracking matrix (analysing key documents, infrastructure, staffing, etc) • Self-evaluation matrix for providers (looking at performance of clinical staff and leadership) • Performance tracking matrix for service users (community members provide their feedback on how they perceive quality of services) • Action Plan matrix (comes after an interface meeting – a joint plan to address identified priorities)
Implementation of CSC • July 2014 – Oct 2016, MoHCDGEC has supportedimplementation of CSC in 6 regionscovering 1069 facilities. (WB support) • In 2016, developmentof the national guideline for implementation of CSC (draftavailable).- to institutionalise CSC into the health system (ownership, costeffectiveness) = sustainability, • GIZ has supported MoHCDGEC to implement CSC in the catchment area of 18 dispensaries.
Results • CSC was highly appreciated and accepted by service providers and CHMTs. • The action plans for the 18 Facilities/Villages were developed and the implementation started immediately.
Results • Many of challenges raised during CSC process were addressed by the community members and village leadership themselves. • Implementation of Community Score Card has also improved collaboration between service providers and users. • Commitment of CHMT to uptake identified priorities into CCHPs but also plan future implementation on their own.
Highlights • BumbuliDC – installment of security doors in lab room - 375,000 raised during the meeting. • Mchakama village, Lindi DC – 2,000,000 contribution by village government purchase solar pannelsin their dispensary. • Mikuvavillage, NanyumbuDC, - about 4 million shillings and materials have been solicited by the community to elevate dispensary into HC - CHMT have committed to budget for the project in the 2017/18 CCHP.
Lessons learnt • To ensure sustainability and scalability of CSC, a cost-effective and clear guideline needs to be elaborated and made available. • For the CSC process to be successful, involvement of all key actors from regional to village level is vital. • Proper orientation and training is needed especially to coordinators of CSC within CHMTs. • The quality and neutrality of facilitators needs to be ensured through careful selection and their training has to be organized well in advance of the implementation. • Engaging citizen as well local Ward and Village government provides an opportunity for raise funds for improving the quality of health services outside the allocated health budget.
Way Forward • Presentation in the TWG 1 and DPG Health Meetings • Finalisation of the national guideline and facilitators’ manual (printing costs) • Institutionalization of CSC in the local government health system; • Orientation to key actors at regional, district, ward and village level (orientation workshops) • Training of facilitators • MoHCDGEC and PORALG to advocate for implementation of CSC and monitoring results in all LGAs • need for a circular • Include CSC as assessment criteria during CCHP reviews – link to planning circle