Download
1 / 44
540 likes | 1.12k Vues
Training Cholesterol. January 2017. Contents. Introduction Overview blood lipids What is cholesterol? Biosynthesis of cholesterol What are triglycerides? Functions of triglycerides Lipoproteins Components of lipoproteins Classification and characteristics of lipoproteins

E N D
Training Cholesterol January 2017
Contents Introduction Overview blood lipids What is cholesterol? Biosynthesis of cholesterol What are triglycerides? Functions of triglycerides Lipoproteins Components of lipoproteins Classification and characteristics of lipoproteins Functions of lipoproteins HDL and LDL: „Good“ and „bad“ cholesterol Train your brain Atherosclerosis Cardiovascular diseases Atherosclerosis pathogenesis Atherosclerosis risk factors Genetic risk: Lipoprotein a 18. What affects cholesterol levels? 19. Cholesterol levels 20. Types of hyperlipidemia 21. High cholesterol: a silent killer 22. Diagnosing elevated blood lipid levels 23. Train your brain 24. Treatment of high cholesterol levels 25. Lifestyle modification 26. Lifestyle modification: Diet 27. First line cholesterol lowering drugs: statins 28. Intensity of statin therapy 29. Second line: Ezetimibe 30. Cholestyramine, Colestipol, Colesevelam 31. 2013 ACC/AHA Guideline 32. High triglycerides: Elevated risk of CVDs? 33. Treatment of high triglyceride levels 34. Triglycerides lowering drugs 35. Triglycerides lowering drugs: mechanisms of action
1. Introduction • Raised cholesterol • increases the risk of cardiovascular diseases • is responsible for a third of ischaemic heart diseases globally. • is estimated to cause 2.6 million deaths (4.5 % of total) globally per year. In 2008, the global prevalence of raised total cholesterol among adults was 39 %.
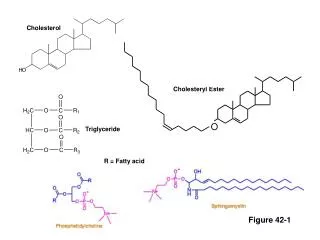
2. Overview blood lipids • “Lipids“ are fat-soluble substances that circulate in the blood. • The two major lipids are • cholesterol • and triglycerides. Both cholesterol and triglycerides belong to the blood lipids, but they have different chemical structures and provide different and important functions in the human body. In excess they can be harmful.
3. What is cholesterol? • Cholesterol is a sterol(connected rings of carbon atoms). • It is essential for maintaining a healthy body as it is • important component of every human cell membrane • maintenance of structural integrity and modulation of membrane • fluidity. • precursor substance for the formation of vitamin D, bile acids and various hormones (cortisol, aldosterone and sex hormones). 25 % 75 % Cholesterol in our body comes from two sources: It is synthesized by the liver and is absorbed from food, yet to different degrees. Cholesterol is only found in products of animal origin.
4. Biosynthesis of cholesterol Hydroxymethylglutaryl-CoA (HMG-CoA) acetyl-CoA Enzyme HMG-CoA reductase Simva-Denk Statins Rosuvastatin Denk 75% mevalonate isopentenyl-pyrophosphate 19 steps squalene cholesterol lanosterol
5. What are triglycerides? A triglyceride consists of three molecules of fatty acid combined with a molecule of the alcohol glycerol. Types of fatty acids • Saturated fatty acids • Trans fatty acids • Created in an industrial process that adds hydrogen to liquid plant oils to make them more solid. • Found in processed food. • Unsaturated fatty acids • Liquid at room temperature. • Largely contained in food of plant origin. • Solid at room temperature. • Largely contained in food • of animal origin.
6. Functions of triglycerides • Triglycerides are the major form of fat and • used by your body as energy source for your • muscles and organs. • They also help to keep the body warm. • In case of excessive dietary intake, triglycerides • are stored in fat cells for future use. Food Like Cholesterol, triglycerides in our body come from two sources: They are synthesized by the liver and are found in many foods. Especially meats, dairy products and plant oils are rich in triglycerides.
7. Lipoproteins • Since lipids are not soluble in water, they have to be bound to protein for the transport within the blood plasma. • These packages are called “lipoproteins”, the protein itself “apolipoprotein”. • There are five main classes: • High-density lipoprotein (HDL) • Low-density lipoprotein (LDL) Differentiations: • Very low-density lipoprotein (VLDL) density, size, composition • Intermediate-density lipoprotein (IDL) • Chylomicrons apolipoprotein + lipid = lipoprotein cholesteryl ester cholesterol triglycerides
8. Components of lipoproteins • Atherogenic lipoproteins are carried on ApoB. • Plasma ApoB levels reflect total number of • atherogenic particles. • Antiatherogenic lipoproteins are carried on ApoA.
9. Classification and characteristics of lipoproteins Lipid content [%] The higher the ratio of protein to lipid content, the higher the density.
10. Functions of lipoproteins HDL LDL lipoprotein lipase IDL VLDL lipoprotein lipase Chylomicrons
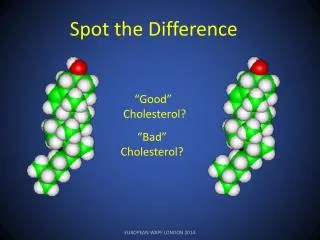
11. HDL and LDL: “Good” and “bad” cholesterol • HDL helps remove excess cholesterol from cells, tissues and arteries. • Transports cholesterol back to the liver. • Reduced risk of atherosclerosis. • LDL delivers cholesterol to cells that need it. • LDL↑: can build up in the walls of arteries • Increased risk of atherosclerosis. video
12. Train your brain • What is the difference between HDL and LDL cholesterol? • HDL-C: higher density and smaller size than LDL-C. • Different functions: LDL-C delivers cholesterol from the liver to body cells • increased risk of atherosclerosis. • HDL-C helps remove excess cholesterol by transporting it back to the liver. • Why is cholesterol important for maintaining a healthy body? • Component of cell membranes; precursor substance for the formation of • vitamin D, bile acids and various hormones. • Name the two sources of cholesterol and triglycerides in your body. • Production in the liver; absorption from food.
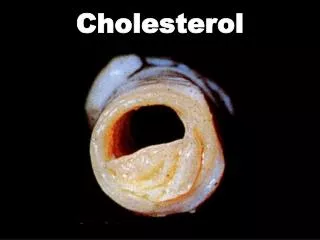
13. Atherosclerosis Atherosclerosis is an inflammatory process in which plaque builds up inside the artery walls, causing thickening and loss of elasticity. It develops over many years and is responsible for a large proportion of cardiovascular diseases (CVDs). Smooth muscle cells • Plaque • narrows arteries, leading to reduced or blocked blood flow. • can rupture and cause blood clots to form inside the artery • all blood flow through the artery can suddenly be blocked. • CVDs may develop based on which arteries are affected. fibrin Cellular waste products Fatty substances Cholesterol
14. Cardiovascular diseases • Coronary heart disease • angina pectoris • heart attack (myocardial infarction) Peripheral artery disease Stroke CVD is the leading global cause of death
15. Atherosclerosis pathogenesis • Factors involved: • LDL-C • vascular damage • cells of the immune system video
16. Atherosclerosis risk factors raised LDL-C and/or low HDL-C, raised triglycerides diabetes older age atherosclerosis smoking obesity high blood pressure (≥ 140 mmHg) physical inactivity genetics Modifiable Non-modifiable
17. Genetic risk: Lipoprotein a • Produced in the liver. • Composition: LDL particle associated with the apolipoprotein(a). • Contributes further to narrowing of the arteries. • Raised Lp (a) is seen as an independent risk factor for the development of atherosclerosis. The plasma concentration of Lp(a) is genetically determined and cannot be influenced by lifestyle changes.
18. What affects cholesterol levels? older age gender Unhealthy diet: rich in cholesterol, saturated fats, trans fats LDL-C ↑ HDL-C ↓ smoking obesity • others: • certain diseases: hypothyroidism, kidney and liver diseases • certain drugs physical inactivity genetics
19. Cholesterol levels Recommended levels for people without any risk factors. • To convert cholesterol levels • mg/dl= mmol/l * 38.6 • mmol/l = mg/dl ÷ 38.6 • Total cholesterol score = LDL + HDL + 20% triglycerides • Cholesterol ratio= Total cholesterol ÷ HDL • Ratio should be < 5. • Optimum ratio is 3.5.
20. Types of hyperlipidemia • Primary lipid disorders (familial) • cause very high levels of cholesterol. This condition can cause patients to get cardiovascular diseases while still young. • Secondary lipid disorders (acquired) • due to lifestyle: excessive dietary intake (saturated fats, • trans fats, cholesterol), physical inactivity, obesity, smoking • diabetes and other diseases • certain drugs • alcohol overuse
21. High cholesterol: a silent killer • High cholesterol typically does not cause any symptoms. • The first sign of high cholesterol could be a cardiovascular event: • angina or heart attack • stroke • pain on walking peripheral artery disease • In rare cases: Appearance of Xanthelasma • depositions of yellowish cholesterol-rich material appearing on the eyelids. • often associated with lipid disorders but may also be idiopathic. • especially in patients with primary lipid disorders
22. Diagnosing elevated blood lipid levels • Total cholesterol • No fasting necessary. • Based on a capillary test. • Includes both LDL and HDL • Risk of CVD development can not be evaluated. • Lipoprotein panel (standard lipid profile) • Based on a venous sample. • Fasting required for 9 to 12 hours. • Total cholesterol, HDL-C, non-HDL-C and triglycerides concentrations. The American Heart Association (AHA) recommends: Have your cholesterol levels checked every fiveyears as part of cardiovascular risk assessment from the age of 20 and more often if your risk is elevated.
23. Train your brain • Name three types of cardiovascular disease. Which process is responsible for their development? • Coronary heart disease (heart attack, angina pectoris), stroke, peripheral artery disease. • Atherosclerosis. • What are risk factors for high cholesterol levels? • Unhealthy diet (saturated fats, trans fats, cholesterol), smoking, physical • inactivity, obesity, genetics, older age, gender, certain diseases and drugs. • What is the difference between primary and secondary lipid disorders? • Primary lipid disorders: due to a genetic defect in lipid metabolism pathways. Very high levels of cholesterol. • Secondary lipid disorders: due to lifestyle, certain diseases and drugs, alcohol overuse.
24. Treatment of high cholesterol levels • Statins First line • Selective cholesterol absorption inhibitors • Bile acid-binding drugs
25. Lifestyle modification Eat a healthy diet, avoiding foods rich in cholesterol, saturated and trans fats. Choose foods rich in unsaturated fats. Reach and maintain a healthy weight. Be physically active. 40 minutes of moderate-to-vigorous-intensity physical activity 3 to 4 times per week (recommended by AHA). Quit smoking.
26. Lifestyle modification: Diet (1) • Saturated fats • mainly contained in foods from animal sources: • some plant-based oils • (palm oil, coconut oil). • Trans fats • Partially hydrogenated oils. • Mainly contained in fried foods and baked goods. LDL-C ↑ HDL-C ↓ LDL-C ↑ • According to the AHA • no more than 5-6% of your total daily calories should come from saturated fats. • no more than 1% of your total daily calories should come from trans fats.
Lifestyle modification: Diet (2) • Cholesterol • Only contained in foods of animal origin. • A daily intake of less than 300 mg cholesterol is recommended. • It is more important to limit saturated and trans fat intake than cholesterol intake. • Unsaturated fats • Mainly contained in fish and foods of plant origin. LDL-C ↓
27. First line cholesterol lowering drugs: Statins • Only cholesterol-lowering drug class directly associated with reduced risk for heart attack and stroke. • Secondary prevention: considerable improvement of cardiovascular mortality. • Relative risk reduction of 20% per 1 mmol/L (38.6 mg/dl) reduction in LDL-C concentration for major vascular events. • Most effective at lowering LDL-C and modest effects on raising HDL (3-15%). 4) Cholesterol reprocessing HMG-CoA reductase rate-limiting enzyme for cholesterol synthesis 3) Increased uptake of LDL-C from the blood into liver cells. 1) Less cholesterol is produced. 2) Cells require more cholesterol. This stimulates the formation of additional LDL-receptors at the surface of liver cells. Mechanism of LDL-C reduction: Simva-Denk Rosuvastatin Denk
29. Second line: Ezetimibe • Cholesterol absorption inhibitor • Inhibits the absorption of dietary and biliary cholesterol. • hepatic LDL receptors ↑ • plasma LDL-C ↓ Monotherapy (when statins are not well tolerated) or in combination with statins when statins alone are not able to achieve the LDL-C target (synergistic).
30. Cholestyramine, Colestipol, Colesevelam • Bile acid sequestrants • Not absorbed, binding of bile acids • excretion of bile acids • increased hepatic bile-acid synthesis • decrease in hepatic cholesterol content • hepatic LDL receptors ↑ • plasma LDL-C ↓ Monotherapy (when statins are not well tolerated) or in combination with statins when statins alone are not able to achieve the LDL-C target (synergistic).
31. 2013 ACC/AHA Guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults
32. High triglycerides: Elevated risk of CVDs? There is evidence that an elevated triglyceride level increases the risk of CVD especially when associated with a low HDL-C level. • Triglycerides measurements correlate with cardiovascular risk, but interpretation of their role is difficult because of multiple confounding associated risk factors (e.g. obesity, diabetes). • Triglyceridesare not directly atherogenic but represent an important biomarker of CVD risk as they are associated with atherogenic remnant particles (VLDL and chylomicron remnants) • VLDL and chylomicron remnants (triglyceride-rich lipoproteins) appear to promote • atherogenesis independently of LDL. • Elevated triglycerides often occur in individuals who are obese, have type 2 diabetes or who drink alcohol excessively. • Very high triglycerides may cause pancreatitis.
33. Treatment of high triglyceride levels • Fibrates • Niacin (Nicotinic acid) • Omega-3 fatty acid ethyl esters
35. Triglycerides lowering drugs: mechanisms of action ω-3 fatty acid ethyl esters Fibrates Niacin - Fibrates ω-3 fatty acid ethyl esters - Niacin - + Fibrates Niacin ω-3 fatty acid ethyl esters
36. Train your brain • Why are statins first-line treatment for lowering LDL-C? • Only cholesterol lowering drug class directly associated with reduced risk for heart attack and stroke. • Secondary prevention: considerable improvement of cardiovascular mortality. • Most effective at lowering LDL-C. • Describe the mechanism of action of statins. • Statins block cholesterol synthesis in the liver. • They act by competitively inhibiting HMG-CoA reductase, the rate limiting • enzyme in cholesterol synthesis. Less cholesterol is produced by the liver. • Decrease in cholesterol concentration causes increased LDL receptor • expression. More LDL-C is taken up by the liver from the blood and is • reprocessed.
Join Denk Pharma Our contributions to keeping you* healthy: • affordable pharmaceuticals for your therapy • German high premium quality for tablets, sachets, • packaging, studies, consultation, availability, support, etc… • raise awareness by conducting Check Up Days (blood glucose, • blood pressure, cholesterol and triglyceride) • constantly enhancing the product portfolio *patients, doctors, pharmacists, sales reps
References • http://www.world-heart-federation.org/heart-facts/fact-sheets/cardiovascular-disease-risk-factors/quick-facts-on-cholesterollipids/ • http://www.sigmaaldrich.com/technical-documents/articles/biofiles/cholesterol-biosynthesis.html • http://www.heart.org/HEARTORG/Conditions/Cholesterol/PreventionTreatmentofHighCholesterol/Know-Your-Fats_UCM_305628_Article.jsp#.WH35PVPhC70 • https://www.rpi.edu/dept/bcbp/molbiochem/MBWeb/mb2/part1/lipoprot.htm • http://www.scientificpsychic.com/health/lipoproteins-LDL-HDL.html • https://www.cholesterin-persoenlich-nehmen.de/Cholesterin/was-ist-cholesterin • http://themedicalbiochemistrypage.org/lipoproteins.php • Talley, Frankum, Currow: Essentials of Internal Medicine 3e. Elsevier, 2015. Third Edition. • „Neue Risikofaktoren“. Ulrike Beisiegel, Prof. Dr. rer. Physiol., Medizinische Klinik, Universitätskrankenhaus Eppendorf, Hamburg. • http://www.lipid-liga.de/images/PDF/Patientenratgeber_Lipoprotein.pdf • American Heart Association: Heart DiseaseandStrokeStatistics. At a glance. 2015. • http://www.world-heart-federation.org/fileadmin/user_upload/images/CVD_Health/Global_CVD_Atlas.pdf • http://www.pfizer.ca/sites/g/files/g10017036/f/201410/Atherosclerosis.pdf • https://www.nhlbi.nih.gov/health/health-topics/topics/atherosclerosis/atrisk • https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3234107/ • http://www.webmd.com/cholesterol-management/tc/high-cholesterol-cause • http://www.mayoclinic.org/diseases-conditions/high-blood-pressure/expert-answers/blood-pressure-medications/faq-20057975 • http://www.cholesterollevels.net/ • https://heartuk.org.uk/files/uploads/documents/huk_fs_mfsP_cholestrigly_leverlsconversion.pdf • http://www.heart.org/HEARTORG/Encyclopedia/Heart-Encyclopedia_UCM_445084_Encyclopedia.jsp?title=cholesterol%20ratio • https://heartuk.org.uk/health-and-high-cholesterol/symptoms-of-high-cholesterol
References http://emedicine.medscape.com/article/1213423-overview http://www.enzyklopaedie-dermatologie.de/artikel?id=4367 http://www.health.harvard.edu/heart-health/making-sense-of-cholesterol-tests https://www.nhlbi.nih.gov/health/health-topics/topics/hbc/diagnosis https://heartuk.org.uk/health-and-high-cholesterol/cholesterol-tests---know-your-number http://www.heart.org/HEARTORG/Conditions/Cholesterol/SymptomsDiagnosisMonitoringofHighCholesterol/How-To-Get-Your-Cholesterol-Tested_UCM_305595_Article.jsp#.WJCT-1PhC70 „Geneticsof Lipid Disorders“. Marija StojanovaJordanov. Springer International Publishing. Switzerland 2015. Mutschler et al.: „Mutschler Arzneimittelwirkungen“. Wissenschaftliche Verlagsgesellschaft. 10. Auflage, 2013. http://www.msdmanuals.com/professional/endocrine-and-metabolic-disorders/lipid-disorders/dyslipidemia http://www.umkelloggeye.org/health-library/zp3086abc http://www.health.harvard.edu/blog/studies-support-broader-use-of-cholesterol-lowering-statins-201507168142 http://www.heart.org/HEARTORG/HealthyLiving/HealthyEating/Nutrition/Saturated- Fats_UCM_301110_Article.jsp#.WJNDhVPhC70 https://www.ncbi.nlm.nih.gov/pubmed/16140878 http://www.heart.org/HEARTORG/Conditions/Cholesterol/PreventionTreatmentofHighCholesterol/Know-Your-Fats_UCM_305628_Article.jsp#.WJNRGFPhC70 http://burdockgroup.com/mechanism-how-trans-fats-raise-cholesterol/ https://www.researchgate.net/publication/47635298_A_mechanism_by_which_dietary_trans_fats_cause_atherosclerosis http://dgk.de/gesundheit/ernaehrung/cholesterinbewusste-ernaehrung/cholesterinmenge-in-lebensmitteln.html https://www.ncbi.nlm.nih.gov/pubmed/16140878
References • http://www.medscape.com/viewarticle/445150 • http://www.health.harvard.edu/blog/studies-support-broader-use-of-cholesterol-lowering-statins-201507168142 • http://www.bmj.com/content/348/bmj.g280 • https://www.ncbi.nlm.nih.gov/pubmed/14692706 • https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2493531/ • http://www.heart.org/HEARTORG/Conditions/Cholesterol/PreventionTreatmentofHighCholesterol/Cholesterol-Medications_UCM_305632_Article.jsp#.WJslZ2_hC70 • http://www.medscape.org/viewarticle/457696_6 • http://www.medscape.com/viewarticle/748727_6 • http://www.heart.org/HEARTORG/Conditions/Cholesterol/PreventionTreatmentofHighCholesterol/Cholesterol-Medications_UCM_305632_Article.jsp#.WJnPTm_hC70 • https://www.ncbi.nlm.nih.gov/pubmed/12822195 • https://lipidworld.biomedcentral.com/articles/10.1186/s12944-016-0286-4 • http://www.medscape.com/viewarticle/439790_2 • http://atvb.ahajournals.org/content/28/11/2016 • https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3875260/ • http://www.medscape.com/viewarticle/573460_5 • http://www.medscape.org/viewarticle/412969_3 • http://www.arznei-telegramm.de/html/2011_10/1110086_01.html