Download
1 / 114
1.54k likes | 4.81k Vues
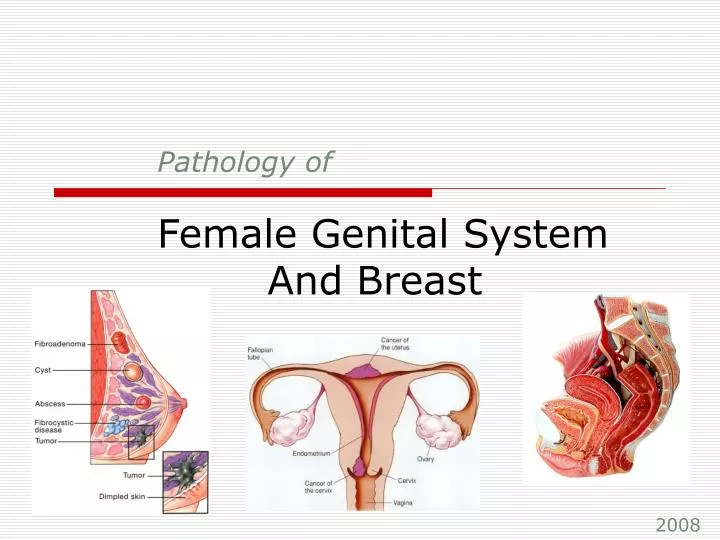
Pathology of Female Genital System And Breast. 2008. Contents: Pathology of. Vulva Vagina Cervix Body of Uterus Fallopian Tubes Ovaries Diseases of Pregnancy Breast. VULVA. Diseases of vulva: Vulvitis (more common but not serious). Non-Neoplastic epithelial disorders.

E N D
Contents:Pathology of • Vulva • Vagina • Cervix • Body of Uterus • Fallopian Tubes • Ovaries • Diseases of Pregnancy • Breast
VULVA Diseases of vulva: • Vulvitis (more common but not serious). • Non-Neoplastic epithelial disorders. • Carcinomas (uncommon but life threatening). • Painful bartholin cysts (caused by obstruction of the excretory ducts of the glands). • Imperforate hymen in children. • Impeding secretions and menstrual flow later in life.
Vulvitis Most important forms of vulvitis related to sexually transmitted disease: • HPV: produce condylomata acuminata and vulvar intraepithelial neoplasia. • Herpes genitalis (HSV1 or 2): causing vesicular eruption. • Gonococcal suppurative infection • Syphilis: produce primary chancre at site of inoculation. • Candidal vulvitis.
Vulvitis Contact dermatitis: the most dommon causes of vulvar pruritus is a reactive inflammation to an exogenous stimulus, whether an irritant or an allergen. • Contact irritant dermatitis: presents as well-defined erythematous weeping and crusting papules and plaques. May be a reaction to urine, sops, detergents, antiseptics, or alcohol. • Contact allergic dermatitis: has similar gross appearance and may result from allergy to perfumes and other additives in creams, lotions, and soaps, chemical treatments on clothing and other antigens.
Non-Neoplasic epithelial disorders • The epithelium of vulvar mucosa may undergo atrophic thinning or hyperplastic thickening • There are two forms of non-neoplastic epithelial disorders: lichen sclerosus and lichen simplex chronicus. • Both may coexist in different areas in the same person, and both may appear macroscopically as depigmented white lesions, referred to as leukoplakia.
Non-Neoplastic epithelial disorders • Lichen Sclerosus: Characterized by atrophic epithelium, usually with dermal fibrosis. Pathogenesis is uncertain, autoimmune reaction may involved Carries an increased risk of developing squamous cell carcinoma. • Lichen Simplex Chronicus End reaction of many inflammatory dermatoses, marked by epithelial thickening, expansion of stratum granulosum and surface hyperkeratosis. Generally, there is no inrecased predisposition to cancer, but suspiciously, lichen simplex chronicus is often present at margins of established cancer of the vulva.
Non-Neoplastic epithelial disorders Lichen Sclerosus Lichen Planus It’s benign dermatoses Lichen simplex chronicus
Tumors • Condylomas and low-grade vulvar intraepithelial Neoplasian (VIN) Condylomas fall into two distinctive biologic forms: • Condylomata lata: (not commonly seen today), are flat, moist, minimally elevated lesions that occur in secondary syphilis • Condylomata accuminata: (more common) may be papillary and distinctly elevated. They occur anywhere on the anogenital surface. Significant characteristic cellular morphology is: perinuclear cytoplasim vacuolization. Vulvar cndylomas are not pre-cancerous but coexist with foci of intraepithelial neoplasia in vulva (VIN grade 1) and cervix.
Condylomas Giant condyloma accuminata A vulva chancre and condylomata
Tumors (continued …) • High-grade vulvar intraepithelial neoplasia and carcinoma of the vuvla • Carinoma of vulva represent about 3% of all genital tract cancers in women. • 90% of vulvar carcinomas are squamous cell carcinomas; and 90% of them are HPV related, and most common seen in relatively younger patients. • Non-HPV-related vulvar squamous cell carcinoma occorus in older women; It is well differentiated and unifocal, and is associated with lichen sclerosus or other inflammatory conditions.
Extramammary Paget Disease • Like that of breast, is essentially a form of intraepithelial carcinoma. • Unlike breast, vulvar Paget disease have no demonstrable underlying carcinoma. • Microscopically, red, scaly plaque; characterized by spread of malignant cells within the epithelium, occasionally with invasion of underlying dermis
A 62 year old woman presented with stenosis (narrowing) of her introitus and symmetrical atrophic changes of the labia. A biopsy showed thinning of the epidermis with replacement of the underlying dermis by dense connective tissue. These findings are most consistent with: Moderate dysplasia (VIN II) Squamous hyperplasia Condyloma acuminatum Verrucous carcinoma Lichen sclerosis A 75-year old woman presents with a pruritic vulvar lesion. Physical examination reveals an irregular white, rough area involving her vulva. If this leukoplakia is due to lichen sclerosis, then biopsies will most likely reveal Atrophy of epidermis with dermal fibrosis Epidermal atypia with dysplasia Epithelial hyperplasia and hyperkeratosis Individual malignant cells invading the epidermis Loss of epidermis pigment Review Questions
VAGINA • The vagina is seldom the site of primary disease; more often it is secondarily involved in the spread of cancer or infection arising in cervix, vulva, bladder, or rectum. • The only primary disorders discussed here are a few congenital anomalies, vaginitis, and primary tumors. • Congenital anomalies are uncommon and include entities such as total absence of vagina, a separate or double vagina, and congenital small lateral Gartner duct cysts arising from persistent embryonic remnants.
Vaginitis • Relatively common clinical problem that is usually transient and not serious. • A large variety of organisms are implicated; in adults, primary gonorrheal infection of the vagina is uncommon; However, it may occur in newborn born to infected mothers. • The frequent organisms are Candida Albicans and Trichomonas vaginalis. Candidal vaginitis produces a curdy white discharge, it is present in about 5% of normal adults, and so the appearance of symptomatic infection always involves predisposing influences or sexual transmission of new aggressive strains.
Vaginitis (continued…) • T. vaginalis produces a watery, copious green discharge, in which parasite can be identified microscopically. • However, T. vaginalis can also be identified in 10% of asymptomatic women, and so symptomatic infection usually represent a sexually transmitted new strain. • Nonspecific atrophic vaginitis may be encountered in postmenopausal women with preexisting atrophy and thinning of the squamous vaginal mucosa.
Vaginal intraepithelial neoplaisa and squamous cell carcinoma • Extremely uncommon, usually occur in women older than age 60 years. • Risk factors are similar to those for carcinoma of the cervix (discussed later). • Associated with HPV infection in most cases. • Vaginal clear cell adenocarcinoma, usually encountered in young women in their late teens whose mothers took diethylstilbestrol during pregnancy; overall risk is 1 per 1000 of those exposed in utero. • Vaginal adenosis, are small glandular or microcystic inclusions appear in vaginal mucosa, appear as red glandular foci lined by mucus-secreting cell; from such inclusions rare clear cell adenocarciona arises.
The most frequent malignancy of the vagina is: Embryonal rhabdomyosarcoma Clear cell adenocarcinoma Vaginal adenosis Sarcoma botryoides Squamous cell carcinoma Vaginal adenosis is most likely to precede the development of Condyloma acuminatum Cervical carcinoma Clear cell carcinoma Carcinoma of the endometrium Squamous carcinoma of the vagian Review Questions
CERVIX • Cervix is often the seat of disease. • Fortunately, most cervical lesions are relatively banal inflammation • But cervix is also the site of the most common cancers in women; squamous cell carcinoma.
Cervicitis • At birth, the columnar mucus-secreting epithelium of the endocervix meets the sqamous epithelial covering of the exocervix at the external os; not visible by naked eye. • In young women, squmocolumnar junction comes to lie visibly on the exocervix (condition called extropion). • In adult, regeneration of both squamous and columnar epithelium in region known as the transformation zone. Frequently, overgrowth of these epithelium blocks the orifices of endocervical glands in the transformation zone to produce small nabothian cysts.
Cervicitis (contiued …) • Inflammation of the cervix are extremely common, and are associated with purulent vaginal discharge. • These inflammation can be infectious or noninfectious cervicitis. • Microorganisms often present are indigenous, incidental vaginal aerobes and anaerobes, streptococci, staphylococci, enterococci, Escherichia coli, Chlamydia trachomatis, Ureplasma urelyticum, T. vaginlais, Candida spp., Neisseria gonorrheae, herpes simplex genitalis, and HPV. • Many of these organisms are transmitted sexually, so cervicitis may represent sexually transmitted disease. Among these organisms, C. trachomatis represent 40% of cases of cervicitis encountered in sexually transmitted disease clinics.
Tumors of the cervix • Cervical carcinoma is one of the major causes of cancer-related deaths in women, despite improvements in early diagnosis and treatment. • Since introduction of the Papanicolaou (Pap) smear 50 years ago, the incidence of cervical cancer has plummeted. • The pap smear remains the most successful cancer screening test ever developed. • Over the same period, the incidence precursor cervical intraepithelial neoplasia (CIN) has increased to more than 50,000 cases annually. It is important to know that nearly all invasive cervical squamous cell carcinoma arise from epithelial changes CIN.
Cervical intraepithelial Neoplasia • Cytologic examination can detect epithelial changes (CIN) before the development of an overt cancer by many years. However, only a fraction of cases of CIN progress to invasive carcinoma. • The peak incidence of CIN is about 30 years, whereas that of invasive carcinoma is about 45 years. • Risk factors for the development of CIN and invasive carcinoma are: -Early age at first intercourse -Multiple sexual partners -Male partner with multiple previous sexual partners -persistent infection by ‘‘High-risk’’ HPV They point to the likelihood of sexual transmission of a causative agent, in this case HPV.
Cervical intraepithelial Neoplasia Left, normal epithelium. Right, CIN2/3 Strongly positive staining nuclie Normal squamous epithelium of the cervix. There is weak positive cytoplasmic staining
HPV (additional information) • High-risk HPV types: 16, 18, 45, and 31, account for the majority of carcinomas, smaller contributions by HPV33, 35, 39, 45, 52, 56, 58, and 59. The viral DNA integrates into the host genome and express E6 and E7 proteins which inactivate tumor suppressor genes p53 and RB, respectively. • Low-risk HPV types: 6, 11, 42, 44 which produce condylomas; the viral DNA does not integrate into the host genome. • The recently introduced HPV vaccine is very effective in preventing HPV infections and cervical cancers. • Many women harbor these viruses, only few develop cancer, suggesting other influences like cigarette smoking and exogenous or endogenous immunodeficiency.
Invasive carcinoma of the cervix • The most common cervical carcinoma are sqamous cell carcinoma 75%, adenocarcinoma and adenosquamous carcinoma 20%, and small cell neuro-ednocrine carcinoma 5%. • In some individual with aggressive intraepithelial changes, the time interval may be considerably shorter, whereas in other women CIN precursors may persist for life. The only reliable way to monitor the course of the disease is with careful follow-up and repeat biopsies. • The relative proportion of adenocarcinoma has been increasing in recent decades; glandular lesions are not detected well by Pap smear.
Invasive carcinoma of the cervix (continued…) • advanced cases of cervical cancer are invariably seen in women who either have never had a Pap smear or have waited many years since the prior smear. Such tomors may be symptomatic, called to attention by unexpected vaginal bleeding, leukorrhea, painful coitus, and dysuria. • Detection of precursors by cytologic examination and their eradication by laser vaporization or cone biopsy is the most effective method of cancer prevention. • Invasive carcinomas range from microscopic foci of early stromal invasion to grossly conspicuous tumors encircling the os. Tumors encircling the cervix and penetrate into the stroma produce a “barrel cervix”, which can be identified by direct palpation.
Risk factors for cervical cancer include all of the following except: Multiple sexual partners A male partner with multiple previous sexual partners Endocervical polyps Early age at first intercourse Cigarette smoking All of the following are significant causes of acute or chronic cervicitis EXCEPT: Gonococci Lactobacilli Chlamydia Mycoplasma Herpes Review Questions
Which of the following statements concerning carcinoma of the cervix is true? A. Stage II disease is confined to the cervix B. Distant metastases accounts for most deaths C. Peak incidence is 20 to 25 years D. 85% associated with human papillomavirus E. Definitive diagnosis is made by Pap smear A 31 year old woman was found to have abnormal cells on pap smear a separate sample of which were sent for HPV (human papillomavirus) typing. Which of the following HPV types would put her at highest risk for subsequent development of squamous cell carcinoma of the cervix? (From additional information) A. 6 B. 11 C. 16 D. 42 E. 44 Review Questions
Multiple small mucinous cysts of the endocervix that result from blockage of endocervical glands by overlying sqmaous metaplastic epithelium are called: Bartholines cysts Chocolate cyst Follicular cyst Gartners duct cyst Nabothian cyst Review Questions
BODY OF UTERUD Many disorders of this organ are common, often chronic and recurrent, and sometimes disastrous. Only the more frequent and significant ones are considered here. • Endometritis • Adenomyosis • Endometriosis • Dysfunctional uterine bleeding and endometrial hyperplasia • Tumors
Endometritis • Can be seen with pelvic inflammatory disease. • It may be associated with foreign bodies or retained tissue subsequent to miscarriage or delivery. They act as a nidus for infection. Removal of the foreign body and offending tissue typically results in resolution. • Endometritis is classified as acute or chronic based on whether there is a predominant neutrophilic or lymphoplasmacytic response, Generally the diagnosis of chronic endometritis requires the presence of plasma cells. Acute endometritis is frequently due to N. gonorrhoeae or C. trachomatis.
Endometritis (continued …) • Endometritis may present with fever, abdominal pain, menstrual abnormalities, infertility and ectopic pregnancy due to damage to the fallopian tubes. • Granulomatous endometritis: seen in immunocompromised individuals in U.S, and in other countries where tuberculosis is endemic.
Adenomyosis • It is the growth of basal layer of the endometrium down into the myometrium. • Endometrial stroma, glands are found well in the myometrium between the muscle bundles. • The uterine wall often becomes thickened and the uterus is enlarged. • Because they are drived from the stratum basalis of the endometrium, they do not undergo cyclical bleeding. Nevertheless, adenomyosis may produce menorrhagia, dysmenorrhea, and pelvic pain before the onset of menstruation.
Endometriosis • It is characterized by endometrial glands and stroma in a location outside the endomyometrium. It may present as a pelvic mass filled with degenerating blood. • Regurgitation theory: (currently most accepted theory) proposes menstrual backflow through the fallopian tubes with subsequent implantation. Indeed, menstural endometrium is viable and survives when injected into the anterior abdominal wall.
Endometriosis (continued …) • Manifestations depend on the distribution of the lesions. Extensive scaring of the oviducts and ovaries produces discomfort in the lower abdominal quadrants, and eventually causes sterility. Pain on defecation reflects rectal wall involvement, and dyspareunia (painful intercourse) and dysuria reflect involvement of the uterine and bladder serosa, respectively. • Almost in all cases, there is severe dysmenorrhea and pelvic pain as a result of intrapelvic bleeding and periuterine adhesions.
Common locations of endometriosis within the pelvis and abdomen
Dysfunctional uterine bleeding • Abnormal bleeding in the absence of a well-defined organic lesion in the uterus is called dysfunctional uterine bleeding. It depends somewhat on the age of the women. • Various causes can be segregated into four groups: - Failure of ovulation.Leads to an excess of estrogen relative to progesterone. - Inadequate luteal phase.Corpus luteum fail to mature normally, leading to relative lack of progesterone. - Contraceptive-induced bleeding.Induce a variety of endometrial responses, e.g. decidua-like stroma and inactive, non-secretory glands. - Endomyometrial disorders. Including chronic endometritis, endometrial polyps, and leiomyomas.
Endometrial hyperplasia • An excess of estrogen relative to progestin, induce hyperplasia, which can be preneoplastic. • They can be classified into simple hyperplasia, complex hyperplasia and atypical hyperplasia. The risk of developing carcinoma is dependent of the severity of the hyperplastic changes. • Potential contributors include failure of ovulation, prolonged administration of estrogenic steroids, polycystic ovaries (estrogen-producing ovarian lesion) cortical stromal hyperplasia, and granulosa-theca cell tumors of the ovary. • Common risk factor is obesity, because adipose tissue processes steroid precursors into estrogens.
Tumors • They tend to produce bleeding as the earliest manifestation. • Endometrial polyps: sessile, usually hemispheric. Histologically, composed of endometrium resembling the basalis, frequently with small muscular arteries. More often they have cystic dilated glands, but some have normal endometrial architecture. They may occur at any age, but more commonly, they develop at time of menopause. clinical significance: - production of abnormal uterine bleeding. - risk of giving rise to a cancer (rare).
Tumors (continued…) • Leiomyoma: - The most common benign tumor in females and are found in 30% to 50% of women during reproductive life. More frequent in blacks than in whites. - They are often referred to as fibroids because they are firm. - Estrogens and oral contraceptives stimulate their growth; conversely, they shrink postmenopausally. - They may be entirely asymptomatic, discovered on routine pelvic examination. The most frequent manifestation, when present, is menorrrhagia, with or without metrorrhagia. They may become palpable to the woman or may produce a dragging sensation. - They rarely transform into sarcomas.
Tumors (continued…) • Liomyosarcomas: • Typically arise de novo from mesenchymal cells of the myometrium. • Almost always solitary tumors. • They are frequently soft, hemorrhagic and necrotic. • Diagnostic features include tumor necrosis, cytologic atypia, and mitotic activity. • They present a wide range of differentiation • Recurrence after removal is common with these cancers. • Many metastasize, typically to the lungs. Yielding a 5-years survival rate of about 40%.
Tumors(continued…) • Endometrial carcinoma: The most frequent cancer occurring in the female genital tract in the U.S and other Western countries. • Appears most frequently between the ages of 55 and 65 years. • There are two clinical stettings in which endometrial carcinomas arise: in perimenopausal women with estrogen excess and in older women with endometrial atrophy. (endometroid and serous carcinoma of the endometrium, respectively). • Well-defined risk factors for endometroid carcinoma: obesity-diabetes-hypertension-infertility • These risk factors poin to increased estrogen stimulation, and it is well recognized that prolonged estrogen replacement therapy and estrogen-secreting tumors increase the risk of this cancer.
TumorsEndometrial carcinoma: (continued…) • Many of these risk factors are the same as those for endometrial hyperplasia, and endometrial carcinoma frequently arises on a background of endometrial hyperplasia. • These tumors are termed endometrioid because of their similarity to normal endometrial gland. • Breast cancer occurs more frequently in women with endometrial cancer than by chance alone. • Two familial cancer syndromes that have an increased risk of the endometrioid type of endometrial carcinoma: • hereditary nonpolyposiscolon cancer syndrome. • Cowden’s syndrome (carries an increased risk of carcinoma of the breast, thyroid, and endometrium, have mutations in PTEN, a tumor suppressor gene).
TumorsEndometrial carcinoma: (continued…) • Serous carcinoma of the endometrium typically arises in a background of atrophy, sometimes in the setting of an endometrial polyps. • Mutations in DNA mismatch repair genes and PTEN are rare in serous carcinoma; however, nearly all cases have mutations in the p53 tumor suppressor gene. • Marked leukorrhea and irregular bleeding are the fist clinical indication of all endometrial carcinoma. • With progression, uterus may be palpably enlarged, and in time it becomes fixed to surrounding structures by extension of the cancer beyond the uterus. Fortunately, these are usually late-metastasizing neoplasms, but dissemination eventually occurs.
_______Causes enlargement of the uterine wall A. Endometriosis B. Adenomyosis C. Both D. Neither _____ May result in pelvic adhesions A. Endometriosis B. Adenomyosis C. Both D. Neither Review Questions
Endometrial carcinoma risk factors include all except: A Obesity B Hypertension C Diabetes mellitus D HPV infection E Infertility Review Questions
FALLOPIAN TUBES • Salpingitis is the most common disease of the fallopian tubes, almost always as a component of pelvic inflammatory disease. It is almost always microbial in origin. • Non-gonococcal infections are more invasive, penetrate the wall of the tubes, and give rise to blood-borne infections and seeding of the meninges, joint spaces, and sometimes the heart valves. • Salpingitis increase risk of tubal ectopic pregnancy. • All forms of salpingitis may produce fever, lower abdominal or pelvic pain, and pelvic masses. They may result in tubo-ovarian abscess, or tubo-ovarian complex. And damage or obstruction of the tubal lumina may produce permanent sterility.
FALLOPIAN TUBES (continued…) • Primary adenocarcinomas: may be of papillary serous or endometrioid histology. They seem to be increased in women with BRCA mutations. Because the lumen and fimbria of the fallopian tube have access to the peritoneal cavity, fallopian tube carcinomas frequently involve the omentum and peritoneal cavity at presentation.
OVARIES (contents): • Follicle and luteal cysts • Polycystic ovaries • Tumors of the ovary • Surface epithelial-stromal tumors - Serous tumors - Mucinous tumors - Endometrioid tumors - Brenner tumor • Other tumors - Teratomas *Benign (mature) cystic teratomas *Immature malignant teratomas *Specilized teratomas