Download
1 / 27
280 likes | 618 Vues
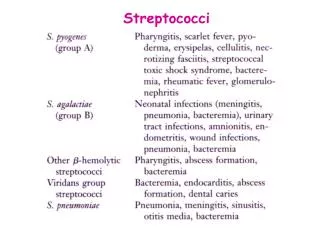
Streptococci Lecture 5. Medical Microbiology SBM 2044. a -haemolytic. non-haemolytic. b -haemolytic. Streptococcus. Gram-positive. Grow in chains. Non-motile. Facultative anaerobes. 3 types of streptococci classification:.

E N D
StreptococciLecture 5 Medical Microbiology SBM 2044
a-haemolytic • non-haemolytic • b-haemolytic Streptococcus • Gram-positive • Grow in chains • Non-motile • Facultative anaerobes • 3 types of streptococci classification: • Early studies distinguished 3 broad groups on blood agar • Group-specific antigens (Lancefield classification) – by serological reactivity of extracted cell wall antigens (A U) • Species – biochemical tests
M-type specific antigen was sensitive to proteases M proteins Streptococcus pyogenes • Natural habitat: Humans • Strains distinguished by M serotyping • Devised by Lancefield in 1920s, using panels of absorbed sera • to hot-HCl extracted antigen, she called “M antigen” • > 100 distinct M types of GAS distinguished since then • - called M1, M2, M3, M4,……..etc. • Highly versatile pathogen • Suppurative infections • Toxinogenic diseases • Immunologically-mediated diseases
GAS diseases – changing patterns • Changes in virulence of prevailing GAS strains ? • Changes in social conditions – less crowding? • Reemergence of severe invasive infections • Sporadic cases since mid-1980s – new virulent strains? • Streptococcal toxic shock • Some cases associated with obviously severe tissue infections • Many others – shock following mild or unapparent infections • Sporadic – implies predisposing factors
Group A Streptococci Principle sites of infection: Invasive infections Local spread (e.g.) Other tissues Pharyngitis, tonsillitis, otitis media, sinusitis. Pharynx Bacteraemia or septicaemia Skin pyroderma, erysipelas Occasionally Streptococcal Toxic Shock Extensive necrosis (necrotizing fasciitis) Deep-seated tissues • Puerperal fever (childbirth fever) in women – major killer in past
Streptococcus pyogenes Tonsillitis Follicular tonsillitis
Streptococcus pyogenes Impetigo Erysipleas Cellulitis
Streptococcus pyogenes Necrotizing fasciitis (< 24 hours post surgery)
Streptococcus pyogenes Scarlet fever
Group A Streptococci • Encounter • Carriers appear asymptomatic • Person-to-person spread is mediated by respiratory droplets or by direct contact to skin • Entry • For pyodermal infections, streptococci need to gain entry into deeper layers of skin • In pharyngeal infections, to prevent from being swept away, GAS must adhere to lipoteichoic acid (LTA), protein F and/or M protein
M protein • Important for cell adherence to keratinocytes • Prevent opsonization by complement • bind to fibrinogen and interferes with the alternative pathway • bind with host complement control proteins and inhibit opsonins formation • Hypervariable regions of M protein are antigenic, but there are > 100 M protein serotypes
EM showing the M Proteins (hair-like surface structures) of S. pyogenes
Group A Streptococci • Spread and multiplication • Most GAS remain localised to the site of initial infection • In pharynx and tonsils, may result in erythema and exudate associated with strep throat • Peritonsillar abscess (quinsy) or spread to adjacent structures (mastoid and middle ear) • Impetigo in skin • Erysipelas and cellulitis in deeper layers of skin • GAS may spread laterally in deep tissues, by secreting enzymes • necrotizing fasciitis and myositis
GAS virulence factors – Excreted products • Both lyse wide range of cells, including PMNs • suppuration and/or necrosis • Cytolytic toxins • Streptolyxin O (SLO) Produced by all strains • Streptolysin S (SLS) • Various subtle effects at sub-lytic concentrations • SLO – ‘sensitive’ to O2 • SLS – stable in O2 b-haemolysis “Thiol-activated” toxin
SLO- and SLS-defective mutants • murine s.c. model - weight loss at 24h post infection Sterile ~3 x 108 cfu ~3 x 106 cfu + 0.5 ~3 x 107 cfu ~3 x 105 cfu ~3 x 109 cfu 0.0 - 0.5 - 1.0 Weight gain (grams) - 1.5 - 2.0 - 2.5 sloΔ1- sagBΔ1 sagBΔ1 sloΔ1 WT PBS
Hyaluronic acid capsule • Antiphagocytic structure on bacterial surface • Hyaluronic acid is abundant in human connective tissue - hence GAS can camouflaged themselves • But capsule may interfere with the adherence of GAS to epithelial cells • so GAS shed the capsule during the early stages of infection using hyaluronidase
Damage • GAS can evoke an intense inflammatory responses in tissues • Streptococcal pyrogenic exotoxins (SPE) • SPE A, B and C cause rash, a characteristic of scarlet fever • SPE A and C are bacterial superantigens that activate a large subset of T cells • Immunologically mediated disease (nonsuppurative sequelae) • acute rheumatic fever (ARF) • acute post-streptococcal glomerulonephritis
Toxic Shock • In past – probably linked to scarlet fever • Since mid-1980s – associated with ‘new’ highly virulent strains - rapidly fulminating • some cases in previously healthy young adults, no obvious • predisposing factors • Associated with production of superantigenic toxins, but other factors also involved
Acute rheumatic fever (ARF) • autoimmune disease - triggered only by GAS pharyngitis • associated with strong immune response to GAS. • antibodies and/or T cells X-react with host antigens? (later) • Symptoms arise > 10days + after GAS infection • responsible GAS strain already ‘cleared’ • Symptoms may include: • inflammation multiple sites, starting with major joints (arthritis) • neurological disorders (Sydenhams chorea) • rheumatic heart disease (RHD) (ca 50% cases) • - damage to heart valves, permanent scaring in survivors
Acute rheumatic fever (ARF) • Initial attack rates low (3% in untreated pharyngitis) • High recurrence (up to 50%) - increasing in severity Widespread prescription of penicillin for ‘sore throats’ Remarkably, GAS have not (yet ?) developed resistance to penicillins
GAS infections - complications Post-streptococcal acute glomerulonephritis (PSGN): • Common, but rarely life-treating - some GAS infections • of either pharynx or skin. • Symptoms arise some 10 days after infection • reflect kidney dysfunction, probably involving inflammation • of glomeruli • Pathogenesis: • Most probably entrapment of GAS antigen-host antibody • complexes at basement membranes of glomeruli • might also involve an ‘autoimmune’ response
Normal glomerulus Glomerulonephritis Mesangial cell Mesangial cell intrusion Endothelial cell, has 100 nm pores PMN Basement membrane Inflammation Too much large immune complex entrapment ? Small complexes diffuse thro’ basement membrane into urine, but the occasional larger complex can’t & is normally removed by mesangial cell Example: Sequel of some S. pyogenes infections
Treatment and Prevention • Penicillin – 10 day oral therapy • Erythromycin or other macrolide antibiotics for individuals allergic to penicillin
Group B streptococci • Streptococcusagalactiae are aerobic G+ diplococci that are β-haemolytic on blood agar plates • found in lower GIT and female genital tracts • GBS is a leading cause of neonatal sepsis and meningitis • prevent opsonization and phagocytosis with a polysaccharide capsule
Enterococci • Enterococcusfaecalis cause UTI, wound infections, endocarditis, intraabdominal abscesses and bacteremia. • Normal flora of GIT and GUT • resistant to bile and high salt concentrations • nosocomial infections • resistance to many antibiotics, often bacteriostatic • bacterial killing must use a combination treatment of a β-lactam and an aminoglycoside