Download
1 / 1
10 likes | 163 Vues
# 460 Anti-angiogenic therapies for metastatic colorectal cancer (MCRC): Preliminary results of a systematic review and meta-analysis A. D. Wagner 1 , D. Arnold 2 , A. Grothey 3 , J. Haerting 4 , S. Unverzagt 1

E N D
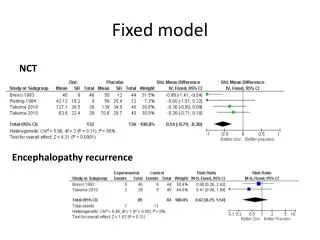
# 460 Anti-angiogenic therapies for metastatic colorectal cancer (MCRC): Preliminary results of a systematic review and meta-analysis A. D. Wagner1, D. Arnold2, A. Grothey3, J. Haerting4,S. Unverzagt1 1 Coordinating Centre for Clinical Trials, Martin-Luther-University Halle-Wittenberg, Germany / Multidisciplinary Oncology Center, Lausanne, Switzerland 2 Department of Medicine IV, Martin-Luther-University Halle-Wittenberg, Germany, 3 Mayo Clinic College of Medicine, Rochester, MN, USA 4 Institute of Medical Epidemiology, Biostatistics and Informatics, Martin-Luther-University Halle-Wittenberg, Germany Figure 1. Hazard ratios for progression-free survival analyzed with fixed effect model. A meta-analysis was therefore performed for trials including bevacizumab (bev) only. When both first- and second- line studies were pooled (5 studies, 3085 pts), the resulting HR for PFS (HR 0.68, 95% CI 0.63-0.74) and OS (HR 0.73, 95% CI 0.73-0.87) confirm significant benefits for the patients treated with bevacizumab. The corresponding differences in weighted mean PFS were 2.7 months and weighted mean OS 2.6 months. The difference in weighted mean RR were 6% between treatment groups. Background Anti-Angiogenesis is one of the most exciting approaches in drug development. However, results from individual trials in MCRC are highly variable and the clinical value of this strategy needs further clarification. Therefore, our objective was to assess the effect of targeted anti-angiogenic therapies in addition to chemotherapy (ctx) in patients (pts) with MCRC. Methods: This systematic review and meta-analysis were performed on the basis of a previously published protocol (Wagner et al., Anti-angiogenic therapy for metastatic colorectal cancer. The Cochrane Library 2007, Issue 4). Progression-free (PFS)- and overall survival (OS) were primary endpoints, with OS being hierachically lower ranked.Response rates (RR),toxicity and secondary resectability were secondary endpoints. Search strategy: Electronic and manual searches in: The Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, proceedings from ECCO, ESMO, ASCO until November 2007. No language limits. Selection criteria: Randomized controlled trials in patients with histologically confirmed MCRC were included. Abstracts or unpublished data were included only if full information as well as final results have been confirmed by contact to the first author. Interventions were systemic, oral or intravenous, targeted anti-angiogenic therapies, in combination with chemotherapy.Agents which have been approved for other indications and were subsequently reported to have anti-angiogenic activity, as well as agents primarily targeting the EGF-receptor, have not been included in this review. Data synthesis: As individual patient data was not provided, aggregate data had to be used for the analysis. Summary statistics for the primary endpoints are hazard ratios (Cox 1972) and their 95% confidence intervals. Table 1: Relevant trials Table 2. Methodological quality Figure 2. Hazard ratios for overall survival analyzed with fixed effect model. Table 3: Grade ¾ Toxicities: pooled results in trials + vs –bev. Conclusions The addition of bevacizumab to chemotherapy significantly improves PFS and OS in MCRC, although the initially observed magnitude of the treatment effect could not be reproduced in later studies. While hypertension, arterial thrombembolic events, cerebral ischemia and proteinuria (all grade ¾) were significantly increased in patients treated with bevacizumab, all-cause 60-day mortality and treatment-related deaths showed non significant differences between patients treated with and without bevacizumab. Main results At present, published data from randomized controlled trials on anti-angiogenic therapies for MCRC is available for bevacizumab (bev) (4 trials in 1st line, 1 in 2nd line) and PTK787-ZK222584 (1 trial in 1st line) only. For a second study on PTK787-ZK222584 as second line therapy, final survival results are still pending. * published as abstract only/ ** only significant differences reported Hurwitz 2004: Follow up every 6 weeks in the first 24 weeks, every 12 weeks thereafter. Considering the median PFS for IFL (6.2 months) and IFL+bev. (10.6 months), systematic bias due to the later registration of progression events in the group treated with IFL+bev is likely Saltz 2007: Study initially planned for the comparison of Xelox/Folfox, later amended to a 2 x 2 factorial design +/- bev. Significant survival difference between trial arms +/- bev only for Xelox +bev, but not for Folfox +bev (Cassidy, ECCO 2007) [Supported by BMBF [FKZ 01 KG 0603] Complete references available at: Dorothea.wagner@chuv.ch