Download
1 / 41
440 likes | 909 Vues
The Lumbar Puncture: This (Really) Is Spinal Tap. Outline. Indications and contraindications Use of CT scan Procedural technique Potential complications Initial CSF studies and interpretation Initial management of meningitis. History of LP. 1891 by Heinrich Irenaeus Quincke

E N D
Outline • Indications and contraindications • Use of CT scan • Procedural technique • Potential complications • Initial CSF studies and interpretation • Initial management of meningitis
History of LP • 1891 by Heinrich Irenaeus Quincke • German Internist born in 1842 • Died in Frankfurt in 1922 • Designed to treat neonatal hydrocephalus • Now a famous rock band (Spinal Tap) Quincke H. Ueber Hydrocephalus. Verhandl Cong Inn Med. 1891;10:321.
Indications • The time to do an LP is the time when you wonder, “should I do an LP?” • Particularly if you’re considering encephalitis or meningitis. • SAH (if the CT is normal) • Meningitis/Encephalitis • Inflammatory polyneuropathies • MS, Guillan-Barre, etc. • Carcinomatous meningitis, tuberculous meningitis • CSF disorder (hydrocephalus, NPH, pseudotumor cerebri) • Therapeutic (i.e., intrathecal chemo, anesthesia) • Injection for myelography
Contraindications • Increased ICP • Exam: Papilledema, focal neurologic exam • Historical concerns: recent trauma/seizures • Focal infection at the LP site • Severe Coagulation defects • Abnormal Anatomy/Mass • Spinal Fracture • Spinal Hardware can be a relative contraindication
Head CT • Never let a head CT delay the institution of antibiotics (30 minute treatment time). • Head CT for subarachnoid, not meningitis • Study by Gopal in Arch Int Med 1999: • 15% with CT had an abnormality, but only 2.7% with a lesion that contraindicated LP • Three clinical Predictors pre-LP: • Altered mental status • Focal Exam • Papilledema
301 Patients • Risks Factors for Mass Effect on CT • Age >60 • Immunocomprimised • History of CNS disease/tumor • Neurologic Abnormality • Seizure • Depressed mental status • NPV 97% • Other 3% did not have issues with LP
Indications for a head CT • Increased ICP • Altered MS, papilledema, focal neuro exam • History of recent head trauma or new seizures • Immunosuppression • Neutropenia, HIV • Recurrent meningitis • Recent OM, sinusitis for possible parameningeal focus (relative)
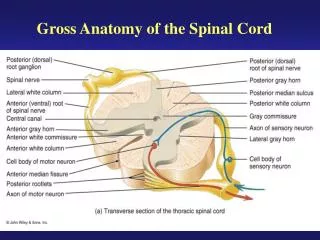
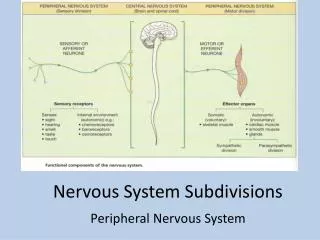
Procedural technique • Goal is to sample the CSF from the subarachnoid space at L3-L4 or L4-L5. • Nerve roots of the cauda equina are at this level, but they are simply pushed over. • The spinal cord usually ends at L1-L2.
Needle route • Skin • Supraspinous and interspinous ligaments • Ligamentum flavum • Epidural space • Dura • Subarachnoid membrane and space
Procedural steps • H&P, consider need for pre-LP CT scan • ABX +/- steroids? • Informed consent • Gather your materials • LP kit • Cleaning solution (Betadine or Chlora-Prep) • Extra Lidocaine • Sterile Gloves • Extra sterile tubes (if necessary) • Chux pads • Extra Needle (atraumatic or smaller gauge) • Consider procedural sedation • Diazepam 5mg, Lorazepam 1mg, Midazolam 1mg
Positioning, Positioning, Positioning • Lateral decubitus position or sitting • Fetal position to widen space between the spinous processes • This is key • Palpate the iliac crests to locate L4/L5, use thumbs to locate • Make an indentation with a pen cap, or other device • Mark should not wash off
Procedural steps • Open the kit. • Pour betadine into tray, drop extra needles, etc • Put on sterile gloves. • Prepare the area in a circular fashion with betadine or povidone-iodine. • Drape. • Inject 1-2% lidocaine at the site.
Needle Position • Bevel parallel or perpendicular to spine? • Parallel! • Bevel should be parallel to dural fibers • Less cutting and more separation • Reported 50% decrease in post-LP headache
Procedural steps • Wait 3-5 minutes for the anesthetic effect • Introduce needle parallel to the bed, bevel perpendicular to spine, in a 30-45 degree cephalad angle • Progress through the layers slowly • Feel the “pop” going into the subarachoid space. • Don’t count on this… • Remove the stylet and look for CSF • Some remove stylet once in intraspinus ligaments
Troubleshooting • Needle angle • Bone spur? • Positioning?
Procedural steps • Attach the manometer (instruct patient to relax) and check the opening pressure • Collect four tubes of 2-5cc of CSF • Replace the stylet and remove the needle • A strand of arachnoid may be drawn out with needle • 600 patient RCT (Strupp NEJM 1997) showed 3x reduction in headache (16% vs. 5%, p<0.005) • Put a bandage at the site and remain supine for 2 hours • Non-significant benefit in several studies
Alternate Needles • Newer ‘atraumatic needles’ • Sprotte needle designed in 80s • Now made by a company called ‘Pajunk” Sprotte G, Schedel R, Pajunk H, et al. An “atraumatic” universal needle for single-shot regional anesthesia: clinical results and a 6 year trial in over 30,000 regional anesthesias. Reg Anaesth 1987;10:104–108.
Atraumatic Meta-Analysis • Lenaerts used 20 G “Yale” instead of Quincke • Obviously, a poor study • Friends don’t let friends associate with Yale
Atraumatic Insertion • Atraumatic cannot penentrate skin very well • Also is more flexible • Can use 18 gauge as guide
Potential complications • Brain herniation • If you get neurologic changes, remove needle immediately • Reverse Trendelenburg, hyperventilate and call Neurosurgery! • Postspinal headache • Most common complication (10-15%) • Use smallest gauge needle possible • Treat with analgesics/epidural blood patch • Caffeine 500mg IV x1 • Local bleeding/infection • Nerve trauma/pain
CSF studies • Tube 1: cell count/diff • Tube 2: protein, glucose, other chem (OCBs, MBP, etc.) • Tube 3: Gram stain, culture, other micro (HSV PCR, etc.) • Tube 4: cell count/diff, cytology • Special studies: Enteroviral, HSV PCR • VDRL, Cocci, Crypto, AFB, Fungal, etc. • Cytology (Presence of CNS malignancy) • Oligoclonal bands, myelin basic protein, etc. • Consider saving an ‘extra tube’ (especially for cytology) • FOR THE LOVE OF GOD, PLEASE HAND-CARRY ALL CSF TO THE LAB YOURSELF.
Accessioning • IF IMPORTANT, DO IT YOURSELF! • In CHCS go to lab tests • Type Now, Ward/clinic collect, STAT • Type CSF • Protein, Glucose, Cell count & Diff, Culture • Type Gram • Sample name ‘CSF’ • Other studies as necessary, may need MMO • Miscellaneous Mail Outs, for Oligoclonal Bands • Ordering these can be a pain in the @$$!!!
CSF interpretation • Opening pressure • Normal 6-18 cm H2O • Falsely elevated in sitting position or a tense patient • Fluid appearance • Fluid should appear clear • SAH: compare tubes 1 and 4; xanthochromia • Xanthochromia should be determined by spectroscopy • We don’t have a spectrometer… So you just look at it
CSF interpretation • Cell count • “Normal” is no more that 5 wbc’s and 1 neutrophil • For bloody taps: 700 rbc/ 1 wbc • If dump the CSF from the manometer, you should be ashamed! • Protein – normal 15/40 mg/dL • 1 mg increase for 1000 rbc’s • Very elevated in infections, mildly elevated in inflammatory disease • Glucose – normal 45-80 mg/dL • Normal is >0.6 of blood glucose level • Ratio of <0.4 has positive LR of 13
CSF Microbiology • If important, look at it yourself! • Gram stain • Always check with Microbiology regarding the gram stain results • 80% positive with bacterial pathogen • GPR: think Listeria! • Cultures • Review plates daily with Microbiology • Call Childrens for HSV, EBV results in 1-2 day
Meningitis: Clinical Presentation • Study by Thomas, et al. CID, 2002 • Headache - 92% • Fever - 71% • N/V - 70% • Photophobia - 57% • Stiff neck - 48% • Seizure - 9% • None were predictive (post-test odds .42-.57)
Examination: Meningitis • Exam: • Petechiae/rash • Genital lesions-usually not present with HSV • Kernig’s: pain with knee extension • Brudzinki’s: flexion of neck leads to hip/knee flexion • Nuchal rigidity • Papilledema not consistent with meningitis alone
Physical examination • Kernig’s: • Sens 5%, Spec 95%, PPV 27%, NPV 72% • Brudzinski’s: • Sens 5%, Spec 95%, PPV 27%, NPV 72% • Nuchal Rigidity: • Sens 30%, Spec 68%, PPV 26%, NPV 73% Absence does NOT r/o disease!
Meningitis • Bacterial: • Strep pneumoniae, N. meningitidis, H. flu, Listeria, GNR’s. • Aseptic: • Viral: enterovirus, HSV, arbovirus, HIV, WNV. • Bacterial: partially treated bacterial, TB • Spirochetes: Lyme, syphilis • Fungi: Cocci, Cryptococcus, Histo
Meningitis • Aseptic: • Amoebae, toxo, rickettsia, others • Drugs: NSAID’s, sulfa, IVIG, INH • Rheumatic diseases (SLE) • Cancer • Sarcoid • Organism depends on: • Age • Medical Conditions/Immune Status • Vaccine History
Bacterial meningitis Neonates: GBS, E. coli/GNRs, Listeria 1-3 Mos.: GBS, Listeria, S. pneumo, H. influenzae 3mo-9 yr.: S. pneumoniae, N. meningitidis 9-50 yr.: S. pneumoniae, N. meningitidis >50 yr.: S. pneumoniae, N. meningitidis,Listeria, GNR’s
Treatment • Droplet isolation for 24-48 hours. • Empiric antibiotics: • Ceftriaxone 2 g IV q12h • Vancomycin 15 mg/kg IV q12h (generally 1-1.5 g IV q12h) • Add ampicillin 2 g IV q4h for coverage of Listeria monocytogenes if patient is >50 years old, immunosuppressed, pregnant, or alcoholic. • Special situations: • Trauma/shunt – cefepime + vancomycin • Immunocompromise – vancomycin/cefepime/ampicillin • PCN allergy – vancomycin/TMP-SMX/+/- chloramphenicol
Treatment • Acyclovir in cases of HSV • +PCR in CSF in cases of meningitis • Empirically in cases of encephalitis • 10 mg/kg IV q8h – maintain good UOP • Steroids • Dexamethasone 10 mg IV q6h • Dose before antibiotics. Reduces TNF. • Increased ICP: • ICU management, elevation of head to 30 degrees, mannitol, hyperventilation to pCO2 of 30mmHg, steroids.
References • Practice parameters: Lumbar Puncture. Neurology, 1993; 43:625 • Special Techniques for neurologic diagnosis in Principles of Neurology, 5th, 1993. New York: McGraw-Hill, p 11-16 • Cooper JR: Routine use of CT prior to lumbar puncture. Br J Rad, 1999; 72:319 • Gopal AK, et al:Cranial CT before lumbar puncture. Arch Intern Med, 1999; 159:2681. • Waldman W and Laureno R: Precautions for lumbar puncture: a survey of neurologic educations. Neurology, 1999; 52:1296.
References • Converse GM, et al: Alteration of CSF findings by partial treatment of bacterial meningitis. J Pediatr, 1973; 83: 220. • Negrini B, et al: Cerebrospinal fluid findings in aseptic versus bacterial meningitis. Pediatr, 2000; 105:316 • Tunkel AR and Scheld WM: Acute bacterial meningitis. Lancet, 1995; 346:1675. • Greenlee JE: Approach to diagnosis of meningitis: Cerebrospinal fluid evaluation. Infect Dis Clin NA, 1990; 4:583. • Quagliarello VJ and Scheld WM: Treatment of bacterial meningitis. NEJM, 1997; 336:708.
References • Flaatten H, et al:Puncture technique and postural postdural puncture headache. A randomized double-blind study comparing transverse and parallel puncture. Acta Anaesth Scand, 1998; 42:1209. • Sharma A: Preventing headache after lumbar puncture. BMJ, 1998; 317:1588. • Nel MR: Epidural blood patching can be used to treat headache. BMJ, 1998; 316: 1019. • Kaplan SL: Clinical presentations, diagnosis, and prognostic factors of bacterial meningitis. Infect Dis Clin NA, 1999; 13:579.