Download
1 / 18
320 likes | 1.34k Vues
Vitamin B12 Deficiency. A practical guide to management in primary care. Plan . Science bit Clinical presentation and complications Investigations Management Discussion of guidelines Mini audit of our patients. Source .

E N D
Vitamin B12 Deficiency A practical guide to management in primary care
Plan • Science bit • Clinical presentation and complications • Investigations • Management • Discussion of guidelines • Mini audit of our patients
Source • Derived from the diet – found in meat, fish, eggs, milk but not in plants • Up to 2yrs worth are stored in the liver.
Causes of B12 deficiency • Impaired absorption • Pernicious anaemia • Gastrectomy • Ileal disease or resection • Malabsorption syndromes • Low dietary intake • Vegans
Pernicious anaemia • Autoimmune disease – antibodies are formed against the parietal cells. This produces atrophic gastritis and reduced IF production. • 1:8000 of over 60s • F>M • All races but more common in fair skin, blue eyed people • Associated with other AA diseases – particularly thyroid diseases, addison’s and vitiligo
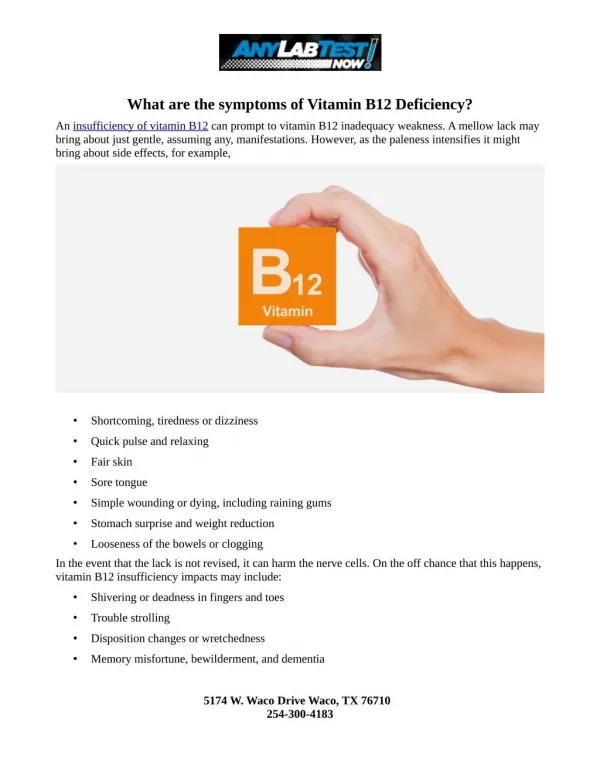
Pernicious AnaemiaClinical features • Slow onset – symptoms of anaemia • ‘Lemon yellow’ colour due to pallor and mild jaundice (due to ineffective erythropoiesis) • Glossitis and angular stomatitis • Neurological changes (B12 <60ng/L) (SCDC) • Glove and stocking parasthaesia • Early loss of vibration sense • Progressive weakness and ataxia • Dementia
Pernicious anaemiaInvestigations • FBC – Megaloblastic anaemia with hypersegmented neutrophils. • B12 levels – low • Parietal cell antibodies - +ve in 90% • Bilirubin may be raised • Serum Folate – may be normal or high • Shilling test • Endoscopy – shows atrophic gastric mucosa
Treatment • B12 Deficiency without neurological involvement: • 1mg Hydroxocobalamin 3 times a week for 2 weeks then every 3 months. • B12 Deficiency with neurological involvement: • 1mg Hydroxocobalamin very other day until no further improvement then every 2months.
Guidelines • Prodigy (CKS) guidelines
Mini – Audit Our Patients • 60 patients with ‘Hydroxocobalamin’ prescribed. • Ave age 70yrs (34-95) • 58% female 42% male
Mini-audit • Do we routinely monitor patients on B12 injections? • Do we consistently give B12 every 3months? • Do we document (or investigate) the cause of the B12 deficiency?
How many injections have they each had over the last 2 years?
Conclusions • We’re a bit inconsistent with monitoring. • We’re a bit inconsistent with dosing. • BUT: Does this simply reflect tailoring tests and doses to patients individual needs? • We should probably pursue the cause of the B12 deficiency (and document this) more often.