Download
1 / 16
170 likes | 778 Vues
ALOPECIA AREATA. DIFICULTADES TERAPEUTICAS Prof. Dra. Lidia E. Valle HOSPITAL GENERAL DE NIÑOS PEDRO DE ELIZALDE. ALOPECIA AREATA. 01/08/97 al 01/08/98 - 6142 1era. Vez 401 p.; 6,52 % patologías del cc y pelo Patologías más frecuentes: tiñas

E N D
ALOPECIA AREATA DIFICULTADES TERAPEUTICAS Prof. Dra. Lidia E. Valle HOSPITAL GENERAL DE NIÑOS PEDRO DE ELIZALDE
ALOPECIA AREATA • 01/08/97 al 01/08/98 - 6142 1era. Vez • 401 p.; 6,52 % patologías del cc y pelo • Patologías más frecuentes: tiñas alopecia difusa alopecia areata • Otras: pediculosis; piodermitis, eccemátides; hemangiomas; falsa tiña; alopecia traumática; nevos; moldes peripilares; querion de Celso; aplasia cutis; psoriasis; miasis. UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
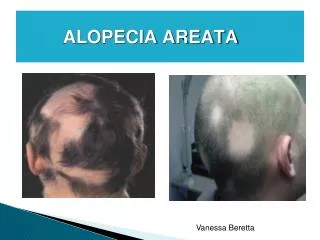
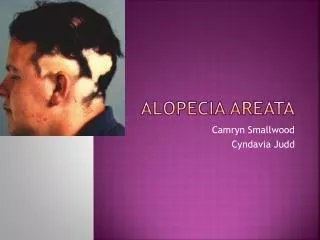
ALOPECIA AREATA • Placa única. • Placas múltiples. • Alopecia areata total de cuero cabelludo. • Alopecia areata universal (c.cabelludo, cejas, pestañas y vellos genitales). UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA • Previo a la terapéutica, considerar: • Antecedentes personales y familiares • Antecedentes de la afección • Tiempo de evolución • Extensión y ubicación de las lesiones • Patologías concomitantes y/o asociadas UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA, terapéutica local • Corticoides locales (cremas, lociones) • Corticoides intralesionales (triamcinolona) • Sustancias irritantes: antralina desde 0,05% al 0,25%; minoxidil al 1% ó 2%; xilol/éter • Sensibilizantes de contacto: dinitroclorobenceno (DNCB); SADBE; difenciprona (DCP) • Tracrolimus UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA, terapéutica EV y vía oral • Pulsos de metilprednisolona EV 5 mg/kg/día por 3 días. • Coticoides vía oral de 1-2 mg/kg/día • Inosiplex 50 mg/kg/día • Ciclosporina 3-5 mg/kg/día • Psoralenos 8-MOP 0,6 mg/kg • Pentoxifilina 20mg/kg/día • Zinc 200 mg/día UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA • No existe un criterio terapéutico unificado • La enfermedad tiene una evolución caprichosa y por lo tanto los resultados son frustrantes para el paciente y poco gratificantes para el médico • El abandono de la terapéutica, la consulta con diferentes profesionales, es frecuente UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA • Los tratamientos locales (corticoides, dncb, antralina, etc.) presentan en oportunidades efectos colaterales • Los corticoides sistémicos también presentan efectos colaterales UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
ALOPECIA AREATA • El tratamiento psicológico considerado pilar fundamental, en oportunidades no es aceptado por el paciente ni por su familia. • Los estudios diversos que se solicitan desorientan al paciente. UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
NUESTRA EXPERIENCIA EN EL ENFOQUE INTERDISCIPLINARIO DE LAS AFECCIONES DERMATOLOGICAS EN NIÑOS Y ADOLESCENTES • 1995-1996 51 casos estudiados en conjunto 22 alteraciones del pelo 20 alopecia areata (17 p.; 3 t.) 2 tricotilomania • 1996-1997 48 casos estudiados en conjunto 13 alteraciones del pelo 12 alopecia areata p. 1 tricotilomania UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE
Fenómeno psicosomático (FPS): la lesión psicosomática no obedece a las leyes del lenguaje y del inconsciente, obedece a una simple alternancia, es algo que se muestra, se desarrolla al lado de la estructura del sujeto. Responde a un estímulo holofrásico interviniendo la función biológica. UNIDAD DERMATOLOGIA PEDIATRICA - ELIZALDE