Download
1 / 23
250 likes | 580 Vues
Oesophagus and Stomach. Phil Thirkell + asfand baig. Anatomy. Blood supply to the oesophagus and stomach? Coeliac artery – a branch off the abdominal aorta Which embryonic structure does the oesophagus derive from? Foregut Endoderm. Histology. Cell Type

E N D
Oesophagus and Stomach Phil Thirkell + asfandbaig
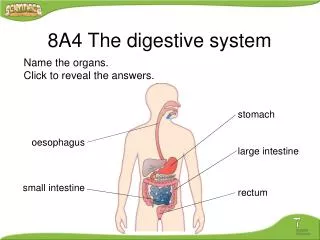
Anatomy • Blood supply to the oesophagus and stomach? • Coeliac artery – a branch off the abdominal aorta • Which embryonic structure does the oesophagus derive from? • Foregut • Endoderm
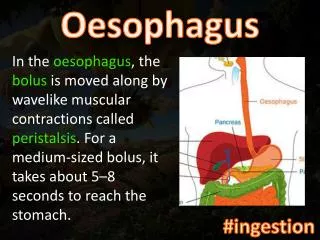
Histology • Cell Type • Non- Keratinised Stratified Squamous Epithelium • Upper 1/3 oesophagus • Striated muscle • Middle 1/3 oesophagus • Striated muscle and Smooth muscle • Lower 1/3 oesophagus • Smooth muscle
Striated Muscle Tubular cells Striations Multiple nuclei Smooth Muscle Narrow, rod shaped cells No striations One nucleus per cell
Gastro-oesophageal Junction • How can you tell where the junction is? • Change from non-keratinised stratified squamous to simple columnar • What forms the lower oesophageal sphincter? • Compression from the diaphragm (right crus) • Angle of entry into the stomach • Intra-abdominal pressure • Mucosal folds (but I don’t know how these help form the junction)
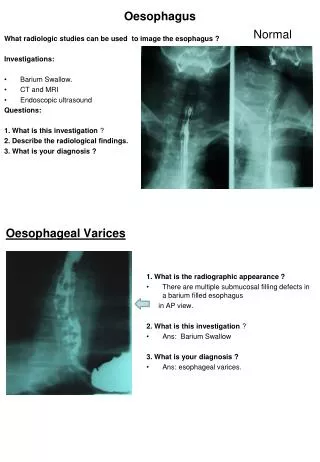
Pathology • Gastro-Oesophageal Reflux Disease • Failure of lower sphincter causes reflux of acid • Oedema/white cell infiltration • Increases risk of cancer • Barrett’s Oesophagus • Metaplasia from stratified squamous to simple columnar • Goblet cells • Produce mucus to protect against acid environment • Considered a pre-malignant condition • Association with adenocarcinoma • Oesophageal Cancer • Late presentation • Can cause obstruction • Poor prognosis • Risk Factors: • Age, male, FH, smoking, alcohol, reflux, Barrett’s, hot drinks • Oesophageal Varices • Dilated veins of portal system • Form due to portal hypertension • Risk of bleeding • Difficult to treat
Stomach • Functions of the stomach? • Storing food • Killing bacteria • Regulate food entry into duodenum • Dissolve and partially digest macromolecules into food • To secrete intrinsic factor • the only indispensable role of the stomach • What are the folds in the stomach? • Rugae – same name for the folds in the bladder, which do the same – allow increase in size without increasing the pressure within
Stomach Secretions • Contents of stomach secretions? • Hydrochloric acid • Enzymes – pepsinogen, gastric lipase • Mucus • Bicarbonate • Water • Intrinsic Factor • Chief cell • Pepsinogen • Parietal cell • HCl • G-cell • Gastrin • Mucus cell • Mucus • D-cell • Somatostatin • ECL-cell • Histamine
Dysphagia • difficulty swallowing • Disease of mouth/tonsils • Inflammation or cancer • Stricture • Pharyngeal pouch • Hiatushernia • Achalasia – problem with peristalsis co-ordination. (sorry to those I told wrong, I was getting confused with oesophageal atresia) • Goitre • Infections (oesophagitis) • Aortic aneurysm
Peptic Ulcer • Causes: • Helicobacter pylori • NSAIDs • Crohn’s disease • Cancer • Zollinger-Ellison syndrome • A non-beta islet cell, gastrin-producing tumour of the pancreas. Loads of gastrin causes huge acid secretion all the time, making patients really prone to ulcers
Peptic Ulcer • Epigastric pain – what happens on eating? • A gastric ulcer gets worse on eating. Food enters stomach, acid is released and it comes into contact with the ulcer, aggravating it and causing pain. • A duodenal ulcer is made better on eating as the pyloric sphincter closes and bicarbonate is released from the pancreas. The pain then starts again after 2-3 hours when the contents of the stomach is released and the acid comes into contact with the ulcer. • Nausea • Bloating/flatulence • Epigastric tenderness • Anaemia – chronic bleeding from the ulcer
Why do NSAIDs cause ulcers? • Normally, prostaglandins are released when gastric mucosa is damaged, causing increased production of mucus and bicarbonate. • Cyclo-oxygenase enzyme 1 (COX-1) creates prostaglandins. • NSAIDs inhibit COX-1, reducing prostaglandin production. This decreases the mucus and bicarbonate secretion • This increases the damage by acid on gastric mucosa ulcers
Stomach Pharmacology • Antacids • Alginates • Bismuth chelates • Prostaglandin analogues • H2 antagonist • Proton pump inhibitors • H. pylori eradication therapy
Antacids • React chemically to neutralise stomach acid (acid + base salt + water + carbon dioxide) • Magnesium hydroxide • Calcium Carbonate • e.g. Rennie • S/E - gas
Alginates • Polysaccharide which reacts with stomach contents to make a raft which floats on the surface to prevent reflux and protects mucosa • E.g. Sodium alginate • Gaviscon is combined antacid and alginate
Bismuth Chelates • Binds pepsin to prevent acid secretion • Coats the mucosa • Increases prostaglandin production • S/E – can cause black tongue and black faeces
Prostaglandin Analogues • Misoprostol • Inhibits acid secretion • Increases mucosal blood flow to generate HCO3 • S/E: diarrhoea and stomach cramps • Can’t be used in pregnancy – causes uterine contractions and can cause a termination • women of child-bearing age should be using contraceptives if prescribed misoprostol as gastric acid treatment
H2-receptor antagonists (anti-histamines) • Blocks the histamine receptor on the parietal cell to reduce acid secretion • e.g. Cimetidine, ranitidine, nizatidine • (not loratidine – only blocks H1, so used in allergies)
Proton Pump Inhibitors • e.g. omeprazole, lansoprazole, pantoprazole • Block the H+/K+-ATPase pump of the gastric parietal cell • Used in patients with reflux, GORD, NSAID ulcers and as 2° prevention in pts who’ve had ulcers • Used to control Zollinger-Ellison until something else can be done about it • Acts systemically, in that it is absorbed into the blood stream, circulates and then acts on the parietal cells – instead of just acting directly on them in the stomach lumen • In acidic conditions the drug can bind to the ATPase, but in neutral conditions it cant. • S/E - ↑risk of infection due to ↓ acid secretion to kill bacteria, decreased vitamin B12absorption due to less acid, decreased calcium absorption. • Nausea + vomiting
H. Pylori eradication • 1 week of: • 1 proton pump inhibitor – omeprazole, lansoprazole • 2 antibiotics – amoxicillin and either: clarithromycin or metronidazole • Can’t use serology to check if the eradication therapy has worked because the antibodies will still be there even if all the bacteria are now dead