Download
1 / 36
370 likes | 484 Vues
N eonatal, Infant , C hild and Mothers Health Family Health. دستاوردهای جهانیان در حمایت از حقوق کودکان و تحقق استعدادهای انسان را بیشتر می توان با بلندی قد کودکان سنجید تا ارتفاع آسمانخراشها . گزارش پیشرفت ملتها2000 یونیسف. اهداف. تعریف خانواده و انواع آن اهمیت پرداختن به بهداشت خانواده

E N D
دستاوردهای جهانیان در حمایت از حقوق کودکان و تحقق استعدادهای انسان را بیشتر می توان با بلندی قد کودکان سنجید تا ارتفاع آسمانخراشها. گزارش پیشرفت ملتها2000 یونیسف
اهداف • تعریف خانواده و انواع آن • اهمیت پرداختن به بهداشت خانواده • تعریف بهداشت خانواده • وظایف و برنامه های مختلف بهداشت خانواده
خانواده • خانواده بعنوان اولين و اساسي ترين نهاد اجتماعي، عبارت است از تجمع مشترك دو يا چند نفر كه به واسطه سببي يا نسبي با هم رابطه زيست شناختي داشته و زير يك سقف زندگي مي كنند و متشكل از والد يا والدين و فرزندان آنان مي باشد و سلامت افراد تحت تأثير اصول، ارتباطات، تكامل اجتماعي ـ شرايط اقتصادي و فرهنگي آن قرار مي گيرند. اعضاء خانواده، مجموعه اي از ژن هاي مشترك هستند و به عنوان واحدي فرهنگي، منعكس كننده فرهنگ اجتماع بزرگتر مي باشند. همچنين خانواده واحدي اپيدميولوژيكي و واحدي براي فراهم كردن خدمات اجتماعي و مراقبت هاي جامع پزشكي است. چگونگي تأثير خانواده بر افراد و يا بالعكس با توجه به تغييرات طبيعي تكامل افراد در طول زندگي و آشنايي با عوامل خطر در خانواده بيشتر مشخص مي گردد.
خانواده اولين محيط اجتماعي است كه فرد در آن قرار مي گيرد و از آن تاثير، مي پذيرد و اين تاثيرپذيري مي تواند از طريق بيولوژيكي و يا رفتاري باشد. تاثير بيولوژيكي خانواده فرد را ممكن است مستعد ابتلاء به بيماري نمايد مانند افسردگي؛ كانسرها و يا تاثير رفتاري مانند پرخوري، عدم تحرّك، اعتياد و الكليسم از طريق الگوي والدين داشته باشد.
چرخه خانواده • خانواده ها پايدار نيستند و همواره درحال تغييرند
انواع خانواده • تنوع ارتباطات افراد، منجر به تشكيل انواع خانواده گرديده است هنوز در اكثر جوامع خانواده سنتي تك هسته اي معمول ترين نوع مي باشد. • واحدهاي خانواده در سرتاسر دنيا شكل هاي متفاوتي دارند. دانشمندان علوم اجتماعي سه نوع خانواده را به شرح زير، تعريف كرده اند : • 1 ـ خانواده هسته اي (Nuclear Family) • خانواده هسته اي يا اوّليه در تمام جوامع انساني، مشترك است و شامل زوجين و كودكان وابسته آنها مي شود. مسئوليت تربيت به عهده والدين بوده و رابطه زوجين، صميمي است. • 2 ـ خانواده گسترده (Extended Family) • يكي از رايج ترين نوع خانواده در خاور دور و خاور ميانه است و بيشتر در مناطق زراعي روستائي، مرسوم است. به طوري كه چند خانواده با رابطه خوني بين مردها باهم زندگي مي كنند، قدرت در دست مرد سالخورده فاميل است، روابط فاميلي بر روابط زناشوئي، ارجح مي باشد و مسئوليت ها تقسيم شده است. • 3 ـ خانواده سه نسلي • خانواده اي كه افراد جوان به دليل نبودن امكانات با نسل هاي قبلي خود به طور موقت زندگي مي كنند. • بديهي است كه انواع مشروع و نامشروع ديگري از خانواده نيز وجود دارد كه در جدول 2 به آن ها اشاره شده است.
بهداشت خانواده • براي دستيابي به بهداشت خانواده بايد مراحل مختلف تكامل، عوامل خطرآفرين در خانواده و عوامل موثر بر سلامت خانواده را شناخت. شماي كلي بهداشت خانواده در شكل 1 نشان داده شده است.
مراحل مختلف زندگي • با وجود تفاوت هاي وسيع در فرآيند تكاملي افراد، وجوه مشترك مشخصي در اكثر موارد در مراحل زندگي وجود دارد و لذا اين مراحل به 6 دوره طبقه بندي مي شود : شيرخوارگي و كودكي، بلوغ و نوجواني، جواني، ميانسالي، از كارافتادگي و پيري.
Women & children make 70% of developing countries population • The 10.6 million annual child deaths are not distributed evenly over the 0-4 year age period • More than 70% of all child deaths occur in the first year of life • And of these … nearly 40% occur in the first month of life (the neonatal period)
More than 42%of total mortality occurs in under 5 children. • Family planning decrease MMR at least 25% • When IMR decreases, desire for child bearing decreases
Only 2 WHO regions account for more than 70% of all under-five deaths: 42% in the African region 29% in South-east Asia region • Only 6 countries account for 50% of all child deaths (2002 data): India (Sear) Nigeria (Afr) China (Wpr) Pakistan (Emr) Ethiopia (Afr) DR Congo (Afr)
What are under-fives dying of?(excluding neonatal causes of death) • Pneumonia • Diarrhoea • Malaria • Measles • HIV/AIDS } ~ 50% Malnutrition contributes to more than half of all under-five deaths
What are neonates dying of? • Preterm births • Severe infection • Asphyxia • Congenital anomalies • Tetanus } ~ 75%
What are mothers dying of? • Pregnancy related bleeding • Pregnancy related infections • Pregnancy related hypertention
Progress has been variable • Neonatal mortality has fallen at a lower rate than post-neonatal or early child mortality • Relatively greater progress has been made in some regions and countries e.g. neonatal mortality is now 58% lower in high income countries than in 1983, compared to 14% reduction in low/ middle income countries • Large variations in mortality rates exist even within the same country
About half of child deaths occur in the neonatal period When do neonates die?
In a developing country, pregnancy related maternal mortality is 38 times more than a developing one. • Every minute in the world, a young woman dies from pregnancy related causes.(585000 annually) • Unplanned and wrongly-spaced pregnancies • compensation of mother,s reservoirs, • the opportunity to take care of child • The ultimate result is child mortality
Crowded family: • higher chidren,s malnutrition, cost of family food • Lower protein & energy and food per capita • Increase in birth order: decrease in IQ and mental capacity • Doubling time of population • Developing: 20-40 years • Developed: 583 years • In Iran as other developing countries marriage rate is very high • 1375 census: more than 45 year old never married • Men 1.7 % • Women 1.6 %
Annual estimated unsafe abortion worldwide: 20 million leads to 76000 young women death mostly in developing countries. Family planning prevents most of these deaths. • Without assessment of pregnancy and essential care leading to maternal and child mortality or irreversible complications. • lactation: lower rate of pregnancy, child health
In Iran, despite family planning activities • 24% of pregnancies are unwanted. • Only 50% of OCP users, use it correctly.
Definition • Family health • Major theme of it is promotion of the quality of life considering family as a unit.
Duties & Programmes of family health office of ministry of health • Mothers • Children • Family planning • Nutrition improvement • Women and Elderly • School health( office of adolescents health and school health)
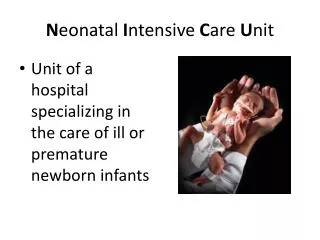
Mothers • Health care before, during & after delivery • Health education • Healthy neonate during first 10 days of life • Safe motherhood • Safe delivery • Maternal mortality • LBW • Premature delivery • MAMAROOSTA
Children • IMCI( Integrated Management of Childhood Illnesses) • مراقبتهای ادغام یافته ناخوشی های اطفال- مانا • كودك سالم • Health care of under 6 y/o children • Height, weight, growth monitoring, nutrition education, vaccination, solid foods, control & treatment of infectious diseases • Neonatal care • Breast feeding
Family planning • Increasing quality & quantity of modern contraception
Nutrition improvement • Prevention of malnutrition, IDA, IDD • IDA: 30% under 5 & female adolescents, 20-50% pregnant women • 1.4% of worldwide mortality( 0.8 million) is related to IDA • Objective: prevention of IDA in 15-49 y/o female and under 5 children. • Education of healthy nutrition in community • 1374: 16% of under 5 moderate & severe malnutrition. • 1377: 13.7% rural & 9.6% of urban children moderate & severe malnutrition. • Controlling parasitic and infectious diseases( preparing the situation for malnutrition)
women • Prevalent cancers: Breast, Cervix • screening: BSE, CBE, Mamography, Pap smear
Elderly • WHO: in 2050 1 in 5 of world population will be elderly. • Iran • 1375: 4.1% • 1378: 5% • 1385: 5.2% • 1390: 5.7% • 1400 estimation: 10 million more than 60 y/o
Drugs • IMCI, family planning, complementary drugs for children
Key messages • Maternal and newborn care and support is essential to achieve a substantial reduction in neonatal mortality • Improving child survival requires coordinated action between maternal and child health, and other programme areas (e.g. EPI, NUT, RBM, HIV) • IMCI is an effective delivery strategy for multiple child survival interventions • For substantive impact, strong community component must accompany the health system strengthening