Download
1 / 24

E N D
AUTOCOIDS By Shiva B.Pharmacy Shiva.pharmacist@gmail.com
INTRODUCTION • Naturally occuring substances – termed as local harmones which originate from diffuse tissues & produce intense pharmacological action near their site of formation & release. • Auto’s=Self ; akos= remedy/ medicinal agent.
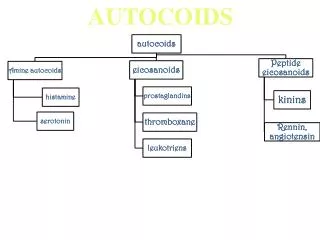
CLASSIFICATION • Based on chemical nature; • 1.BIOGENIC / ENDOGENOUS AMINES: Histamine, 5-HT. • 2.POLYPEPTIDES:Bradykinin, sub-p. • 3.LIPID SOLUBLE ORGANIC ACIDS/ PHOSPHO LIPID DERIVATIVES: • (A).EICOSINOIDS: PG’S, PC’S, LT’S, TX’S. • (B).PAF.
HISTAMINE • Tissue amine. • Histos- Tissue. • DISTRIBUTION: Widely distributed in almost all mammal tissues & in venom of bees & wasps. • SYNTHESIS: In mammals formed by Decarboxylation of Histidine in prescence of Histidine decarboxylase. • STORAGE: Present in platelets, leucocytes, basophills & mastcells. • Mainly in mastcells & basophills due to presence of his.decarboxylase, specialised storage granules.
MECHANISM OF ACTION • Acts through 4 receptors viz : H1, H2, H3, H4 – all belonging to family GPCR. • Activation of H1 receptors : • Activation of H2 receptors:
PHARMACOLOGICAL ACTIONS • CVS: (A). BLOOD VESSELS: In herbivores – Sys & Pul vasoconstriction. • In humans Pul.vasodilation. • Acts by 3 ways: (a).Activation of H1 receptors on the endothelial cells cause rapid- short lived vasodilation. • (b).Activation of H2 receptors in the vascular smooth muscle causes slower but prolonged vasodilation. • (c).Relaxation of smooth muscle of capillaries & venules leading to their dilation and fall in BP.
PHARMACOLOGICAL ACTIONS • (B).BP: Therapeutic doses induces hypotension, short lived. • Large doses –prolonged hypotension. • Hypotension left untreated may cause irreversible shock & death. • Histamine induced hypotension is partially reversed by anti-histaminics & completely reversed by adrenaline.
PHARMACOLOGICAL ACTIONS • TRIPLE RESPONSE; When given (20mcg) ID develops a triple response : • (a).FLUSH(RED REACTION): Red line r spot develop with in 10sec, due to local dilation of capillaries & venules. • (b).WHEAL: Local swelling due to edema, mottled reddening around injury. • Lasts about 1 1/2min. • Due to increased permeability of capillaries 7 post capillary venules with consequent xtravasation of fluid.
PHARMACOLOGICAL ACTIONS • (c).FLARE: Redness with irregular margins spreads out from injury. • Triple response is part of normal reaction to injury. • Its prevention is used to evaluate anti-histaminic activity of a new drug. • (C).HEART:Increases sinus rate (+vechronotropic action) • Increases the amplitude of ventricular contraction (+inotropic effect) • Decreases AV conduction time & increases coronary blood flow, high conc. induce ven.fibrillation.
PHARMACOLOGICAL ACTIONS • (D)SMOOTH MUSCLE: Stimulates smooth muscles of various tissues by direct action(H1). • Bronchial & Uterine smooth muscle – highly sensitive. • GIT & Ureteral smooth muscle – respond moderately. • Thru H1 receptor – gall bladder contraction , • H2 receptor – gall bladder relaxation. • ‘H’ –induced bronchospasm – antagonised by adrenaline, isoprenaline & aminophylline but not by anti-histaminics r atropine.
PHARMACOLOGICAL ACTIONS • ENDOCRINE GLANDS: Important physiological mediator of gastric acid secretion. • CNS: Doesn’t cross BBB, ‘H’ constituted in 2types of cells – Histaminergicneurones & Mast cells. • Considered as ‘Waking amine’- increase in sensitivity of large cerebral areas to excitatory inputs. • IMMUNOMODULATION: Increases Humoral & Cellular immunity by various receptors , H1- cellular immunity , H2- Humoral immunity.
A,D,M,E: • Stable compound & absorbed from all sites . • Rapidly under go first pass metabolism in liver. • Metabolism varies acc.to: animal spcs, sex , organ studied. • Chemically it is B-Imidazolyletylamine. • End products of metabolism include N-Methyl imidazoleaectic acid, N-acetyl histamine.
ADR • Due to pharmacological actions: hypotension, visual disturbances, dyspnea, diarrhoea. • Man, Gunea pig- extremely sensitive. • Rats & Mice – highly resistant. • Large dose causes – severe nausea, gripping, headache & sweating. • USES:Study of gastric acid secretion.
ANTI-HISTAMINICS • Certain phenolic ether – anti-histaminic properties. • CLASSIFICATION: By two ways Clinically & Chemically. • (A).CLINICAL CLASSIFICATION: • 1.POTENT & SEDATIVE: Diphenhydramine, Promethazine. • 2.POTENT & LESS SEDATIVE: Cyclizine, Meclizine. • 3.LESS POTENT & LESS SEDATIVE: Antazoline, Cinnarizine. • 4.NON SEDATIVE: Loratidine, Cetirizine.
CHEMICAL CLASSIFICATION • General formula: • Based on configuration of ‘X’ classified as : • 1. ETHANOLAMINES(X=‘O’): Diphenhydramine, Doxylamine. • 2.ETHYLENE DIAMINES(X=‘N’): Mepiramine, Antazoline.(show negligible anti-cholinergic & anti-emetic efcts) • 3.ALKYL AMINES (X=‘C’): Chloropheneramine, Triprolidine. • 4.PIPERAZINES: (X=‘C’ in conjunction with piperazine ring): Cinnarizine, Cetirizine.
CHEMICAL CLASSIFICATION • 5.PHENO THIAZINES (X=‘N’ as apart of phenothiazine nucleus): Promethazine, Trimeprazine, show potent anti-emetic effect. • 6.PIPERIDINES: Loratadine, Fexofenadine. • 7.DIBENZOXYPINES: Doxepine (Tricyclic anti depressant) shows potent anti-histaminic properties.
‘H’- ANTAGONISTIC ACTIONS • 1.ANTI-HISTAMINIC ACTIONS: Competatively block ‘H’ at various sites. • Antgonize stimulant action of ‘H’ on: Smooth muscle of GIT, bronchi, uterus & bld.ves. • Reduce ‘H’ induced triple response. • Anti-allergic & anti-inflammatory actions involve: (a). Inhibition of release of mediators from mastcells, basophills. • (b).Down regulation of H1-receptors. • Don’t antgonize CVS actions of ‘H’.
ANTAGONISTIC ACTIONS • OTHER ACTIONS: Related to their blocking of 5-HT & A1-Adreno receptors. • 1.SEDATION & HYPNOSIS: CNS depression – common side effect. • Induce varying degrees of sedation, drowsiness & sleep. • 2.CNS STIMULATION: Stimulation is less , conventional doses of Promethazine cause restlessness, tremors & insomnia.
ANTAGONISTIC ACTIONS • 3. ON ANS: First gen. anti-histaminics show muscarinic blocking activity, second gen. anti-histaminics doesn’t show these actions. • 4.ANTI-EMETIC & ANTI-MOTION SICKNESS: Diphenhydramine & Promethazine block histaminergic signals from the vestibular nucleus to vomiting center. • 5.ANTI-PARKINSONIAN EFFECTS: Central anti-muscarinic actions useful in treating parkinsonism.
ANTAGONISTIC ACTIONS • 6.CVS: Rapid IV administration of Diphenhydramine, Antazoline may produce dose related prolongation of QT interval due to membrane stabilising effect. • 7.LOCAL ANAESTHESIA: Promethazine, Diphenhydramine exhibit local anaesthetic activity. • A,D,M,E: Well absorbed orally & parenterally. • Anti-histaminic effect starts with in 15-30 min, peaks by 1hr & lasts for 3-6hrs. • Meclizine- action persists for 12-24hrs.
ANTAGONISTIC ACTIONS • A,DM,E: First gen compounds metabolised by CYP3A4 in liver. • H1-antagonists induce hepatic microsomal enzymes, facilitating their own metabolism. • ADR: Mild, • 1.CNS: Sedation & Hypnosis, Fatigue. • In children less than 2yrs- Promethazine cause Apnoea. • ANTI-MUSCARINIC EFFECTS: Dry mouth, blurred vision, bladder disturbances & rarely impotence.
ADR: • GIT: Nausea, vomiting, epi-gastric distress. • MISC: May produce allergic manifestations despite of their anti-allergic & anti-inflammatory properties.
THERAPEUTIC USES Used in treatment of : 1.Allergic disorders, 2.Reagenic allergy, 3. Allergic conjunctivitis , 4. Mastocytosis, 5.Other uses (a).As hypnotics, (b).As anti-emetics, (c).In parkinsonism, (d).In motion sickness & vertigo, (e).Anti-tussives, (f).Local anaesthetics.