Download
1 / 64
860 likes | 1.62k Vues
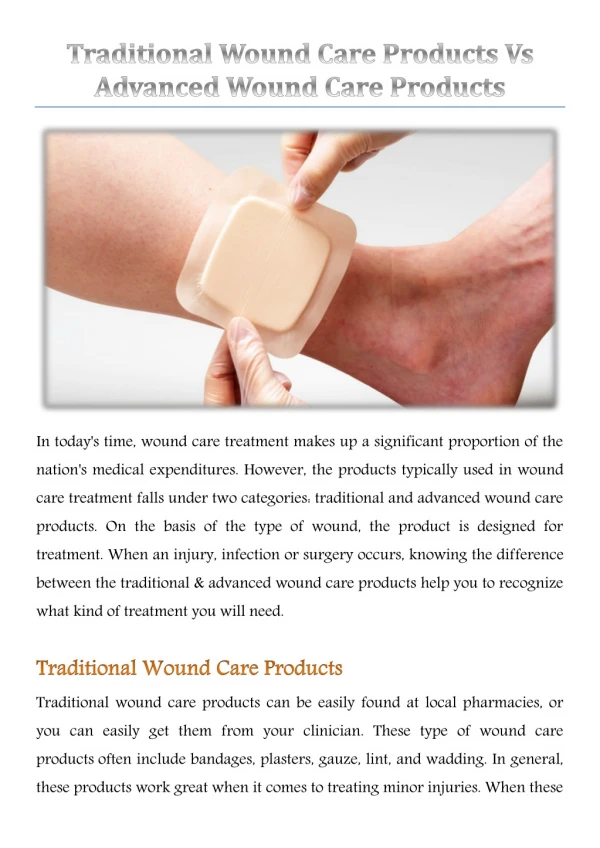
Advanced Wound Care. Wound Healing Process. Acute, Healing Wound. Young, healthy cells Plenty of growth factors Few inflammatory cytokines Low levels of proteases. Treating Chronic Wounds. Prevent & Control Infection Treat/Eliminate Causative Factors Edema Varicose veins Diabetes

E N D
Acute, Healing Wound • Young, healthy cells • Plenty of growth factors • Few inflammatory cytokines • Low levels of proteases
Treating Chronic Wounds • Prevent & Control Infection • Treat/Eliminate Causative Factors • Edema • Varicose veins • Diabetes • Heart disease • Pressure • Malnutrition • Debris/foreign body/necrotic material
Identify Problems Early and Transition to Advanced Wound Care Good Wound Care Advanced Wound Care Growth Factors Bioengineered Tissue NWPT Hyperbaric Medicine Curative Surgery Cellular Tissue Products • History • Assessment • Debridement • Warm, moist environment • Offloading • Topical Care
Holistic Care • Treating the Whole patient versus treating the Hole in the patient
In Addition to Wound Measurements… • Lab Work – CBC, HgbA1C, Albumin • Vascular Testing - Doppler, Angiography, MRA, TCPO2 measures, Arteriogram • Infection Assessment - X-ray, Bone Scan, Tissue Biopsy, MRI • Physical Assessment– Vital Signs, Pain, Weight, Psychological, Community Resources
Chronic, Non-Healing Wounds • Prolonged Inflammation • Bacteria • Foreign Body • Repetitive trauma • Necrosis • Lack of growth factors • High cytokine levels & excess concentration of MMPs
Wound Dressings • Protect from contamination • Prevent trauma • Absorbs drainage • Debrides • Provides medication, moist healing environment, etc. When picking out your dressings, remember the Cardinal Rule: Keep Moist tissue Moist and Dry tissue Dry!
Topical Wound Management Considerations • Wound: depth, presence of slough, moist, dry, painful, infection? • Product: conformability, antibacterial activity, pain, ease of use, fluid handling properties • Patient: activity level, continence, mental status, sensitivity to medicated dressings, fragile skin, lifestyle, compliance, caregiver • Cost: unit cost, reimbursement, availability
Clean Granular Wound Base • Objectives: Protect & keep moist • Treatments: • Hydrocolloid • Hydrogel • Secondary dressing • Vacuum assisted closure (VAC) device • Wet to damp saline (Temporarily)
Clean Deep Wound Crater • Objective: Fill the space with uniform contact • Treatments: • Hydrogel • Alginate • Foam • Hydrocolloid • Vacuum assisted closure (VAC) device • Wet to damp saline (Temporarily)
Slough or Necrotic Wound • Objective: Debride and cleanse • Treatments: • Enzymatic debridement: Santyl Collagenase • Autolytic debridement: hydrocolloid, hydrogel dressings • Pulse irrigation • Wet to damp saline (Temporarily)
High Drainage Wound • Objectives: Absorb and contain • Treatments: • Alginate • Foam • Vacuum assisted closure (VAC) device • Wet to damp saline (Temporarily)
Sinus/Tunnel/Underming • Objectives: Prevent pre-mature closure, absorb exudate • Treatments: Loose packing • Impregnate gauze with hydrogel • Calcium alginate if high drainage • Vacuum assisted closure (VAC) device • Wet to damp saline (Temporarily)
Infected Wound • Objectives: Decrease local bacterial count • Treatments: • Topical antibiotic or antimicrobial • Incision & Drainage • Culture & Sensitivity • Wet to damp saline (Temporarily)
Local Wound Care • Hydrocolloid • Hydrogel • Calcium alginate • Foam • Collagenase • Antimicrobials • Growth factors • Cellular or Tissue Products (Formerly known as Biological Skin Substitutes)
Hydrocolloid • Indications: Venous ulcers, pressure ulcers, diabetic ulcers, 1st and 2nd degree burns • Absorbency and film dressing • Highly absorbent gel (polyurethane) • Oxygen and water vapor permeable • Adhesion and elasticity • Bacterial barrier • Allows for autolytic debridement • Can stay in place for 72 hours
Hydrocolloids Pros: Come in all shapes, sizes, and thicknesses Cons: Must be applied correctly or will roll—choose appropriate size, thickness for location of wound
Hydrogel • Indications: Mildly exuding wounds, clean wounds, partial thickness wounds, pressure, diabetic, surgical • Absorbs 5 times own weight--can absorb a limited amount of exudate. • Cooling soothing effect • Facilitates autolytic debridement • Delivered in many forms • Amorphous gel, Sheets, Strands • Can stay in place for 24 hours
Hydrogels Pros: Hydrogel pads are great for burns, can be very soothing Hydrogels come in all forms Cons: Can be difficult to find and can be costly depending on brand
Calcium Alginates • Indications: Wounds with large amount of drainage • Derived from brown seaweed • Absorbs up to 30 times weight • Will form a gel when comes in contact with exudate • Comes in many forms • Sheets, ropes, loose fibers packs • Maintains a moist wound environment • Can stay in place 24 to 72 hours
Calcium Alginates Pros: non-adhesive, moldable, absorbent, aids in providing Moist Healing environment Cons: If wound isn’t wet enough, will stick
Specialty Absorptive Highly absorptive fiber layers such as cellulose, cotton or rayon Pros: Non-adherent, easy to use, absorbent Cons: May be costly
Foam • Indications: Highly exudative wound requiring a non-stick surface (e.g. venous stasis) • Highly absorbent (20 times weight) • Non-adherent wound contact layer, hydrocellular foam, waterproof outer layer • Can be formed • Cavity, heel, sacral, trach etc. • Allows for autolytic debridement and gaseous exchange • Can be left in place for 72 to 96 hours
Foams Pros: Lots to choose from, provides moist environment, effective with hypergranulation Cons: Can be expensive if exudate requires daily changes
Collagenase Santyl • Indications: A wound requiring debridement of fibrinous exudate, other necrotic material or slough • Debrides necrotic tissue without harming good tissue • Apply once daily • Not recommended for use with Silver products
Antimicrobials • Indications: Infected wounds • Bacterial count greater than 10 5 --decreases wound healing rates • Bacterial proteases degrade growth factors • Topical Silver products • Acticoat • Silvercell • Silvasorb gel • Iodoflex/Iodosorb gel • sustained release of iodine and the desloughing action is provided by the unique cadexomermatrix
Growth Factors Indication: Diabetic foot ulcer • Activates endothelial cells and fibroblasts • Stimulates vascular proliferation, migration, new blood vessel formation • People who use 3 or more tubes of REGRANEX® Gel may have an increased risk from cancer. • Can be very effective • Have a new “360” program to help patients obtain medication and monitor progress.
CollagenOxidized Regenerated Cellulose (ORC) • Indicated in Stalled Wounds • ORC inactivates MMPs and Elastace
Cellular or Tissue Products (CTP) • So many, so little time • Apligraf • Dermagraf • Oasis • Graft Jacket • Primatrix • Integra • And so many more….
Compression & Collagen VSU 4 weeks 7 weeks Day 1 Prisma Silver Foam 3 layer Compression Has decreased more than half in wound surface area Continue same care Resurfaced Measured for Compression Stockings
CTP Oasis Day of application 2 Days post App 4 weeks post initial App VSU Note the carmelization 2 wks s/p 2nd Oasis Application
What is this? Stasis Dermatitis
What type of wound? Arterial
What is the Stage? Stage 1, 5th right sub-met head Stage 1 pressure
When to Refer • No change in size or depth for 2 weeks • Increase in size • Vascular Changes • Necrosis • Infection • Edema • Dehiscence • Foreign Body • Repetitive trauma
Wounds to Refer to Wound Center for Evaluation • Diabetic Ulcers • Pressure Ulcers • Venous Stasis Ulcers • Osteomyelitis • Vascular Insufficiency Ulcers • Delayed Radiation Injury • Burns, Bites and other complex or problem healing wounds
What Is It? • Hyperbaric Oxygen Therapy (HBOT) is breathing 100% oxygen while the entire body is pressurized to a point greater than sea level This is usually 2 to 2.4 absolute atmospheres (the equivalent of the pressure exerted by a 33-45 foot dive into sea water)
2 Mechanisms of Action • Compression of bubbles • Increases Partial Pressures of Oxygen • Hyperoxygenation (O2 carried via plasma) • Vasoconstriction (Reduces Edema) • Angiogenesis (Increases rate) • Antimicrobial(aerobic/anaerobic)
Effects of HBOT on Wound Healing • Oxygen levels remain high • in arterial blood - 2 minutes • muscle - 3 hours • subcutaneous tissues - 4 hours • At tissue PO2 of 30mm Hg: • leukocytes kill bacteria • fibroblast growth begins • collagen is laid down
Typical Treatment Protocol • 100% Oxygen at 2-2.5 ATA • 90 Minutes • 5/days a week • Re-Evaluate every 20 treatments • Up to 60 treatments depending on indication
UHMS Indications for HBOT 1. Air or Gas Embolism2. Carbon Monoxide Poisoning Carbon Monoxide Poisoning Complicated By Cyanide Poisoning3. Clostridial Myositis and Myonecrosis (Gas Gangrene)4. Crush Injury, Compartment Syndrome and Other Acute Traumatic Ischemias5. Decompression Sickness6. Arterial Insufficiencies: Central Retinal Artery Occlusion Enhancement of Healing In Selected Problem Wounds7. Severe Anemia8. Intracranial Abscess9. Necrotizing Soft Tissue Infections10. Osteomyelitis (Refractory)11. Delayed Radiation Injury (Soft Tissue and Bony Necrosis)12. Compromised Grafts and Flaps13. Acute Thermal Burn Injury 14. Idiopathic Sudden SensorineuralHearing
Adjunctive HBOT and Problem Wounds • HBOT is only one component of a comprehensive wound healing program • Non-healing wounds are evaluated to determine underlying conditions which might interfere with healing • More conservative measures should be tried first