Download
1 / 18
370 likes | 2.73k Vues
Pulse. The pulse has been studied for centuries. Information gained: Frequency, regularity Patency of peripheral arteries Characteristics of the arterial pressure pulse wave The arterial pulse contour changes to the periphery:

E N D
The pulse has been studied for centuries. • Information gained: • Frequency, regularity • Patency of peripheral arteries • Characteristics of the arterial pressure pulse wave • The arterial pulse contour changes to the periphery: • Resistance: viscosity, vessel geometry opposes flow; HR independent • Inertia: mass opposes rate of change of flow, HR dependent • Compliance: distensibility opposes changes of blood volume, HR-dependent
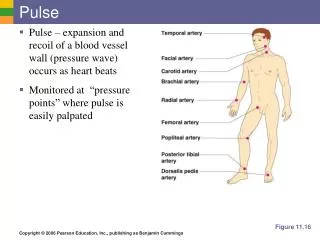
Location of Pulses • Carotid – similar to central aortic pulse (delay of 20msec) • Radial – used to assess the volume and consistency of the peripheral vessels. • Brachial • Femoral • Posterior tibial • Dorsalis pedis • Look for any differences in the pulse amplitude, contour, or upstroke.
Factors Influencing the Pulse • Stroke volume • Rate of ejection • Distensibility of peripheral arteries • Peripheral resistance • Pulse rate • Pulse pressure • Size of the vessel • Distance from the heart
Normal Pulse (1/2) • The normal central aortic pulse wave is characterized by a fairly rapid rise to a somewhat rounded peak. • The anacrotic shoulder, present on the ascending limb, occurs at the time of peak rate of aortic flow just before maximum pressure is reached. • The less steep descending limb is interrupted by a sharp downward deflection, coincident with AV closure, called incisura. • The pulse pressure is about 30-40 mmHg.
Normal Pulse (2/2) • As the pulse wave is transmitted peripherally, the initial upstrokes becomes steeper, the anacrotic shoulder becomes less apparent, and the incisura is replaced by the smoother dicrotic notch.
Abnormal Pulses • Inequality in the amplitude of the peripheral pulses: • Obstructive arterial diseases , most commonly artherosclerosis • Aortic dissection • Aortic aneurysm • Takayasu arteritis (pulseless disease) • Supravalvular aortic stenosis (fixed form of LVOT caused by narrowing of ascending aorta)
Pulsus Parvus • The pressure is diminished, and the pulse feels weak and small, reflecting decreased stroke volume (e.g. heart failure), restrictive pericardial disease, hypovolemia, mitral stenosis, and increased peripheral resistance (e.g. exposure to cold, severe CHF). • Pulsus Parvus et Tardus (weak and delayed): →Aortic Stenosis
Aortic Stenosis (1/2) • LVOT obstruction • Reduces SV, prolongs LV total ejection time, and retards the rate of initial stroke output into the aorta and distal arterial system. • Anacrotic character (anacrotic pulse) • Interruption of the upstroke of the carotid pulse. AS is likely to be hemodynamically significant when the anacrotic notch is felt immediately after the onset of the upstroke.
Aortic Stenosis (2/2) • Delayed upstroke of the ascending limb (pulsus tardus) • Prolonged LV ejection time. • Appreciated by simultaneous palpation of carotid pulse and auscultation fo the interval between S1 and S2. • Normally the carotid pulse occurs closer to S1; in severe AS closer to S2. • Thrill (carotid shudder)
Bisferiens Pulse • Increased arterial pulse with a double systolic peak. • Second peak, the tidal wave, presumed to represent a reflected wave from the periphery. • Causes: hemodynamically significant AR • HCM: rarely palpable; rapid LV ejection during early systole, rapid decline due to LVOT obstruction, and tidal wave from periphery.
Bigeminal Pulse • Normal beat alternating with a premature contraction. • SV of the premature beat diminished, and pulse varies in amplitude accordingly. • May masquerade as pulsus alternans • Causes: decreased BP (e.g. severe HF, hypovolemic shock, cardiac tamponade) and peripheral resistance (e.g. fever), s/p aortic valve replacement. • Present in normal individuals after exercise.
Pulsus Alternans (1/2) • Variation in pulse amplitude occurring with alternate beats due to changing systolic pressure. • When the cuff pressure is slowly released while taking BP, phase I Korotkoff sounds are initially heard only during the alternate strong beats; with further release of cuff pressure, the softer sounds of the weak beat also appear. • Degree of pulsus alternans can be quantitated by measuring the pressure difference between the strong and the weak beat.
Pulsus Alternans (2/2) • Causes: • Left ventricular failure – usually accompanied by a left-sided S3. • May be seen in patients with severe AR • Frequently precipitated by ectopic beats (bigeminal pulse) • Mechanisms: • Alternating preload and afterload, incomplete relaxation, • Change in ventricular contractility, causing changes in end-diastolic volume and pressure.
Pulsus Paradoxus (1/2) • Pressure drop > 20 mmHg during inspiration. • Normally, systolic arterial pressure falls 8-12 mmHg during inspiration. • Evaluated with sphygmomanometer: • when the cuff is slowly released the systolic pressure at expiration is first noted. With further slow deflation of the cuff, the systolic pressure during inspiration can also be detected.
Pulsus Paradoxus (2/2) • Causes: • Cardiac Tamponade • COPD, hypervolemic shock • infrequently in constrictive pericarditis and rescrictive cardiomyopathy. • Mechanism: • Decreased LV-SV due to an increased RV-EDV and decreased LV-EDV during inspiration. • In cardiac tamponade, the interventricular septum shifts toward the LV cavity during inspiration (reverse Bernheim’s effect) b/c of increased venous return to RV, decreasing the LV preload. • Decrease in pulmonary venous return to the LV during inspiration also contributes to decreased LV preload.
Bounding Pulses (1/2) • A.K.A. water-hammer pulse or the Corrigan pulse. • Most commonly in chronic, hemodynamically significant AR. • Seen in many conditions associated with increased stroke volume: PDA, large arteriovenous fistula, hyperkinetic states, thyrotoxicosis anemia, and extreme bradycardia. • Not seen in acute AR, since SV may not have increased appreciably.
Bounding Pulses (2/2) • Physical signs of aortic insufficiency are related to the high pulse pressure and the rapid decrease in blood pressure during diastole due to the AI: • Lighthouse sign (blanching & flushing of forehead) • de Musset's sign (head nodding in time with the heart beat) • Ladolfi's sign (alternating constriction & dilatation of pupil) • Becker's sign (pulsations of retinal vessels) • Müller's sign (pulsations of uvula) • Corrigan's pulse (rapid upstroke and collapse of the carotid artery pulse) • (Watson's) Water-hammer pulse • Quincke's sign (pulsation of the capillary bed in the nail) • Mayen's sign (diastolic drop of BP>15 mm Hg with arm raised) • Rosenbach's sign (pulsatile liver) • Gerhardt's sign (enlarged spleen) • Duroziez's sign (systolic and diastolic murmurs heard over the femoral artery when it is gradually compressed) • Hill's sign (A ≥ 20 mmHg difference in popliteal and brachial systolic cuff pressures, seen in chronic severe AI) • Traube's sign (a double sound heard over the femoral artery when it is compressed distally) • Lincoln sign (pulsatile popliteal) • Sherman sign (dorsalis pedis pulse is quickly located & unexpectedly prominent in age>75 yr)