Download
1 / 86
920 likes | 1.35k Vues
Achieving Perioperative Hemostasis. Jay Kambam, MD, FACA Chief, Cardiac Anesthesia James A. Haley VA Medical Center Tampa, FL & Adjunct Professor of Anesthesiology USF, Tampa, FL & Vanderbilt University Medical Center Nashville, TN. NO DISCLOSURES. May 15, 2012.

E N D
Achieving Perioperative Hemostasis Jay Kambam, MD, FACA Chief, Cardiac Anesthesia James A. Haley VA Medical Center Tampa, FL & Adjunct Professor of Anesthesiology USF, Tampa, FL & Vanderbilt University Medical Center Nashville, TN NO DISCLOSURES May 15, 2012
PERIOPERATIVE HEMOSTASIS • Normal hemostasis is a complex interaction between vessel wall, platelet function, plasmatic coagulation, and fibrinolysis. • Causes of perioperative coagulopathy and bleeding are multifactorial • Because of PCI and Stents, multiple antiplatelet drugs and thrombin inhibitors are increasingly being used • Understanding the details of perioperative hemostasis and pharmacodynamics of drugs involving hemostasis is essential Jay kambam
Hemostasis • Blood must be fluid • Must coagulate (clot) at appropriate time • Rapid • Localized • Reversible (fibrinolysis) Thrombosis…inappropriate coagulation (Examples: DVT, Stent Thrombosis) Jay kambam
HEMOSTASIS:3 Major systems involved • Vessel wall vasoconstriction Endothelin • Platelets First Hemostasis Plug Adhesion, Activation, Aggregation (AAA) • Coagulation cascade Second Hemostasis Plug Coagulation factors Plasmin FSP Jay kambam
Hemostasis Vessel Injury Collagen, vWF Endothelin PLATELET ADHESION VASOCONSTRICTION INITIAL RELEASE REACTION ADP SEROTONIN PLATELET AGGREGATION PHOSPHOLIPIDS INCREASED RELEASE REACTION ADP COAGULATION SECOND HEMOSTATIC PLUG FIRST HEMOSTATIC PLUG (FIBRIN PLUG) (PLATELET PLUG) FSP Platelet-fibrin clot Jay kambam
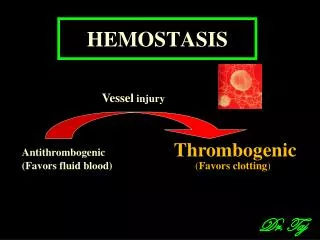
VESSEL WALL - ENDOTHELIUM Vessel injury or FB/Stent, low flow Thrombogenic Antithrombogenic (Favors fluid blood) (Favorsclotting) Anticoagulants Procoagulants Jay kambam
VESSEL WALL Endothelin, Collagen, tPAI, vWF, Factors, PL Prostacyclin, NO, ADPase, tPA, Heparin, Thrombomodulin Jay kambam
Antithrombotic Properties of Endothelium • Anti-platelet properties • Covers highly thrombogenic basement membrane • Uninjured endothelium does not bind platelets • PGI2 (prostacyclin) and NO from uninjured endothelium inhibit platelet binding (anti-Txa2) • ADPase counters the platelet aggregating effects of ADP Jay kambam
Antithrombotic Properties of the Endothelium Anticoagulant & Fibrinolytic properties • Heparin like molecules: activate anti-thrombin III • Thrombomodulin(glycoprotein) - Antithrombin • Binds to thrombin • Decreases ability to produce fibrin • Increases ability to activate Protein C, which inactivates factors Va and VIIIa • Endothelial cells produce tPA which activates fibrinolysis via plasminogen to plasmin Jay kambam
Prothrombotic Properties of Endothelium • Synthesis of von Willebrandfactor (vWF) • Release of collagen & tissue factor (FIII) • Production of plasminogen activator inhibitors (tPAI) • Membrane phospholipids bind and facilitate activation of clotting factors via Ca++ bridges
VASOCONSTRICTION Serotonin causes vasoconstriction Jay kambam
Dense Granule Alpha Granule Jay kambam
Contents of platelet secretary granules and their physiological activities Secretary Granules Physiological activities 1.Alpha Granules Coagulation factors I & VCofactors for coagulation cascade Platelet specific proteins Platelet F4 PF4 potentiates ADP induced aggregation & antiheparin activity Low affinity PF4 LA-PF4 possesses antiheparinactvty Glycoproteins Adhesion and cell to cell interaction 2.Dense Granules ADP and ATPADP stimulates aggregation & secretion CalciumPromotes coagulation SerotoninVasoconstriction Jay kambam
Adhesion, Activation, Aggregation (AAA) Jay kambam
PLATELET FUNCTION AGGREGATION • GPIIb/IIIa- fibrinogen interaction • Key step for hemostasis, part of final common pathway • Therapeutic target of inhibitors Jay kambam
Platelet Activation Pathways Collagen Thrombin PAR-4 ADP Epinephrine P2Y12 Arachidonic acid TxA2 GP1b vWF GP IIb/IIIa Fibrinogen Jay kambam
Second Hemostasis Plug PLASMATIC COAGULATION
Hemostasis Vessel Injury Collagen, vWF Endothelin PLATELET ADHESION VASOCONSTRICTION INITIAL RELEASE REACTION ADP SEROTONIN PLATELET AGGREGATION PHOSPHOLIPIDS INCREASED RELEASE REACTION ADP COAGULATION SECOND HEMOSTATIC PLUG FIRST HEMOSTATIC PLUG (FIBRIN PLUG) (PLATELET PLUG) FSP Platelet-fibrin clot Jay kambam
Intrinsic pathway (PTT) XIIa Extrinsic Pathway (PT) XIa TF IIIa Prothrombin II IXa VIIa VIII VIIIa Xa V Va Soft clot Thrombin IIa Fibrinogen I Fibrin Hard clot XIIIa Fibrin Jay kambam
FINAL STEPS - COAGULATION Jay kambam
Platelet-Fibrin clot Jay kambam
Minimum Fibrinogen Levels Jay kambam
CRYOPRECIPITATE Jay kambam
Transfusion-associated Circulatory Overload (TACO) Jay kambam
Fibrinolysis Plasminogen tPA(Tissue Plasminogen Activator) Plasmin Fibrin Split Products (FSP) Fibrin Jay kambam
FIBRINOLYSIS Jay kambam
Lysine Analog Jay kambam
€Aminocaproic acid & Tranexamic acid Jay kambam
Anticoagulant and Antiplatelet DrugsMechanism of action • PlateletsPrimary Hemostasis Plug Antiplatelet Drugs: TxA2 inhibitors: ASA Thienopyridines(P2Y12/ ADP receptor Inhibitors ): Clopidogrel(plavix), Prasugrel(apagrel), Ticlopidine(Ticlid) GP IIb/IIIa Antagonists: Tirofiban (Aggrastat), Eptifibatide (Integrelin), Abciximab (ReoPro) • Coagulation cascadeSecondary Hemostasis Plug Anticoagulants : Indirect Thrombin Inhibitors: Coumadin, Heparin Direct Thrombin Inhibitors: Lepirudin(Angiomax), Argatroban, Bivalirudin(Refludan),Dabigatran(Pradaxa) Jay kambam
ANTIPLATELET DRUGS - Mechanisms • Aspirin - Thromboxane A2 Inhibitors • Clopidogrel(Plavix) • Prasugrel(apagrel)Thienopyridines • Ticlopidine(Ticlid) • Aggrastat(tirofiban) • ReoPro(abciximab) GP IIb/IIIa Antagonists • Integrilin(eptifibatide) P2Y12/ADP Receptor Inhibitors Jay kambam
Antiplatelet Drugs: Inhibition of activation &/or aggregation Jay kambam
ASPIRIN • Inhibition of Thromboxane A2 production • Orally administered • Rapidly absorbed from GIT • Peak levels observed in about 30 minutes • Irreversible COX type 1 inhibitor • Chew and do! Jay kambam
Thienopyridines:TICLOPIDINE, CLOPIDOGREL & PRASUGREL • Antiplateletagents are used to treat, prevent arterial thrombosis. • Thienopyridine derivatives, inactive in vitro, requiring metabolism to achieve in vivo activity. • Inhibit binding of ADP to platelet receptor(P2Y12). Jay kambam
CLOPIDOGREL Prodrug (Thienopyridine) Administered only orally No direct antiplatelet activity Metabolized in the liver Active metabolite inhibits platelet aggregation Peak concentration of active metabolite is seen in 1 -2 hrs Metabolite binds to platelet P2Y12 receptor and irreversibly inhibits ADP-induced platelet aggregation Jay kambam
PRASUGREL • Prodrug (Thienopyridine) • Ten to 100 times more potent than clopidogrel • Administered only orally • No direct antiplatelet activity • Metabolized in the liver more rapidly (levels 2 times higher) • Faster activity • Active metabolite inhibits platelet aggregation • Peak concentration of active metabolite is seen in 0.5 hr • Metabolite binds to platelet P2Y12 receptor and irreversibly inhibits ADP-induced platelet aggregation Jay kambam
PLATELET INHIBITORS • Aspirin - Thromboxane A2 Inhibitors • Clopidogrel(Plavix) • Prasugrel(apagrel)Thienopyridines • Ticlopidine(Ticlid) • Aggrastat(tirofiban) • ReoPro(abciximab) GP IIb/IIIa Antagonists • Integrilin(eptifibatide) P2Y12/ADP Receptor Inhibitors Jay kambam
GpIIb/IIIa ANTAGONISTS • Platelet GpIIb/IIIa receptors play a pivotal role in platelet-mediated thrombus formation, binding to fibrinogen,vWF & Collagen • IIb/IIIaantagonists differ in receptor affinity, reversibility, and specificity • GpIIb/GpIIIa antagonists more completely inhibit platelet aggregation than do ASA and Theinopyridines Jay kambam
Platelet Activation Pathways Collagen Thrombin PAR-4 ADP Epinephrine P2Y12 Arachidonic acid TxA2 GP1b vWF GP IIb/IIIa Fibrinogen Jay kambam
GP IIb/IIIa Antagonists: Tirofiban (Aggrastat) Eptifibatide (Integrelin) Abciximab (ReoPro) GP IIb/IIIa antagonist Inhibition of platelet aggregation GP IIb/IIIa receptors occupied by antagonists Agonist Fibrinogen ADP, thrombin, collagen, epi Inactive platelet GP IIb/IIIareceptors in unreceptive state Active Platelet Aggregating platelets Jay kambam
Glycoprotein IIb/IIIa inhibitors Tirofiban(Aggrastat) • Nonpeptide • KD 15 nmol/L • Indication: acute coronary syndrome Jay kambam