Download

1 / 20
230 likes | 438 Vues
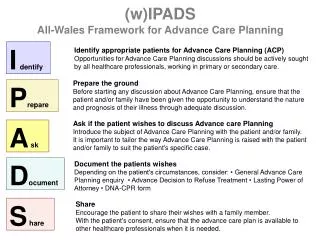
Advance Care Planning (ACP). Tracy Reed RGN, BSc (Hons) DN MSc Queens Nurse Education Facilitator for End of Life Care The Harlow Integrated Team 2nd Floor The Latton Bush Centre Harlow Essex CM18 7BL Mobile no: 07770686994 Email: tracyelizabeth.reed@sept.nhs.uk.

E N D
Advance Care Planning (ACP) Tracy Reed RGN, BSc (Hons) DN MSc Queens Nurse Education Facilitator for End of Life Care The Harlow Integrated Team 2nd Floor The Latton Bush Centre Harlow Essex CM18 7BL Mobile no: 07770686994 Email: tracyelizabeth.reed@sept.nhs.uk
Advance Care Planning (ACP) Advance care Planning (ACP) is a process of discussion between an individual and their care provider irrespective of discipline. The process of ACP is to make clear a person’s wishes and will usually take place in the context of an anticipated deterioration of the individual’s condition. It is recommended that with the individual’s agreement this discussion is documented, regularly reviewed and communicated to key persons involved in their care. National End of Life care programme. 2007 - Advanced care Planning: A guide for Health and Social Care staff.
“All people approaching the end of life need to have their needs assessed and their wishes and preferences discussed.” Peoples choice and control should be central to the delivery of high-quality, end of life care. Image: National End of Life Care Programme. (National End of Life Care Programme, Advance Care Planning: a guide for health and social care staff. February 2007)
Why do it? • Around 500,000 people die in England each year, this will rise to around 530,000 by 2030. • 54% of complaints in acute hospitals relate to care of the dying/bereavement (Healthcare commission 2007). • Only around one third of general public have discussed death and dying with anyone (BBC Mori poll 2005).
Prognostic Indicator Guidance Three triggers that suggest that patients are nearing the end of life are: 1. The Surprise Question: ‘Would you be surprised if this patient were to die in the next year, few months, weeks, days’? 2. General indicators of decline - deterioration, increasing need or choice for no further active care. 3. Specific clinical indicators related to certain conditions.
The Process of Advance Care Planning can be Broken Down into Four Broad Components 1. Opening the conversation? 2. What options might be available to the person? 3. What sort of things might be identified? 4. What methods of recording or communicating wishes are available? The statement is not legally binding but should be used when determining a person's best interests in the event they lose capacity to make those decisions.
What could an ACP conversation include? An ACP discussion might include: • the individual's concerns and worries. • their important values or personal goals. • their understanding about their illness and prognosis. • their preferences for types of care or treatment that may be beneficial in the future and the availability of these. • It’s important to encourage communication. However, sometimes you will need to refer the conversation to someone more qualified.
Advance Decision to refuse Treatment ADRT enables a person aged 18 or over to refuse specific treatment in the future when they have lose capacity. (Previously Known as Living wills or Advance Directives). Must be valid and applicable to current circumstances. Must state which treatment is being refused (they can cancel their decision). Must be in writing • Signed and witnessed. • State clearly that the decision applies even if life is at risk.
Advance Decision to Refuse Treatment - ADRT • Legally binding document. • Formalizing what a person does NOT want to happen to them. • Related to mental capacity and living wills. • Lasting Power of Attorney. • Choice over what a person would like to happen if they can no longer make the decision themselves.
PPC Asks Three Questions • In relation to your health what has been happening to you? • What are your preferences & priorities for future care? • Where would you like to be cared for in the future?
Barriers to ACP and PPC use • Timing- when is the right time to mention it? • Staff characteristics- e.g. discomfort, lack of knowledge, lack of confidence and or training, lack of time to deal with end of life discussions. • Specific challenges of using ACP and PPC with people who have non malignant diseases. • Perceived patient characteristics such as denial. • Family characteristics.
TALKING ABOUT DYING WON’T MAKE IT HAPPEN Some tips: • Be direct. • Acknowledge it’s not an easy subject for many people. • Be clear what is possible and available. • Be sensitive to cues. • Listen to what people are saying. • Allow people time to reflect. • Be prepared to talk about it more than once. www.dyingmatters.org
Summary • ACP is a process which involves talking and thinking about future care/illnesses/life with illness. • It can lead to leaving instructions to help others decide in the event of incapacity. • It can help a person to think about what is important to them as they prepare for illness or the last phase of life, and help them refocus. • Nothing recorded from an ACP discussion should be used in decision making until the person can no longer make current decisions.
DVD ‘I didn’t want that’
‘How people die remains in the memory of those who live on.’ Dame Cecily Saunders Founder of the Modern Hospice Movement