Download
1 / 1
10 likes | 87 Vues
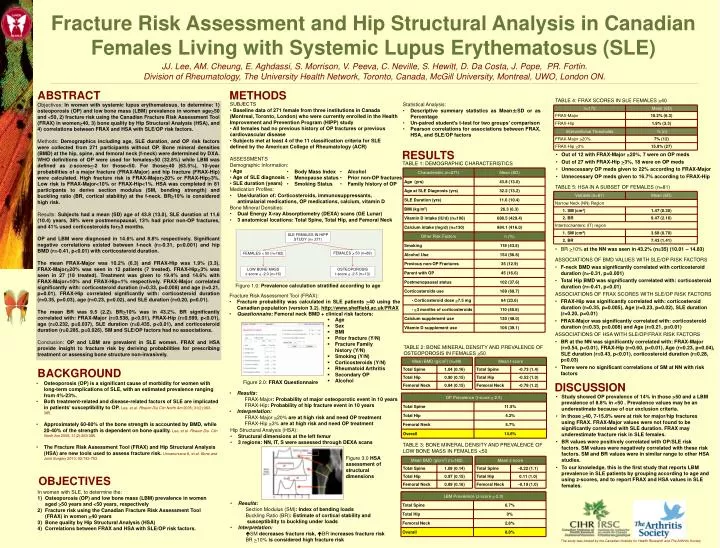
ABSTRACT. METHODS. SUBJECTS Baseline data of 271 female from three institutions in Canada (Montreal, Toronto, London) who were currently enrolled in the Health Improvement and Prevention Program (HIPP) study

E N D
ABSTRACT METHODS SUBJECTS • Baseline data of 271 female from three institutions in Canada (Montreal, Toronto, London) who were currently enrolled in the Health Improvement and Prevention Program (HIPP) study • All females had no previous history of OP fractures or previous cardiovascular disease • Subjects met at least 4 of the 11 classification criteria for SLE defined by the American College of Rheumatology (ACR) ASSESSMENTS Demographic Information: • Age • Age of SLE diagnosis • SLE duration (years) Medication Profiles: • Use/duration of: Corticosteroids, immunosuppressants, antimalarial medications, OP medications, calcium, vitamin D Bone Mineral Densities: • Dual Energy X-ray Absorptiometry (DEXA) scans (GE Lunar) • 3 anatomical locations: Total Spine, Total Hip, and Femoral Neck Objectives: In women with systemic lupus erythematosus, to determine: 1) osteoporosis (OP) and low bone mass (LBM) prevalence in women age>50 and <50, 2) fracture risk using the Canadian Fracture Risk Assessment Tool (FRAX) in women>40, 3) bone quality by Hip Structural Analysis (HSA), and 4) correlations between FRAX and HSA with SLE/OP risk factors. Methods: Demographics including age, SLE duration, and OP risk factors were collected from 271 participants without OP. Bone mineral densities (BMD) at the hip, spine, and femoral neck (f-neck) were determined by DXA. WHO definitions of OP were used for females>50 (32.8%) while LBM was defined as z-scores<-2 for those<50. For those>40 (63.5%), 10-year probabilities of a major fracture (FRAX-Major) and hip fracture (FRAX-Hip) were calculated. High fracture risk is FRAX-Major>20% or FRAX-Hip>3%. Low risk is FRAX-Major<10% or FRAX-Hip<1%. HSA was completed in 81 participants to derive section modulus (SM, bending strength) and buckling ratio (BR, cortical stability) at the f-neck. BR>10% is considered high risk. Results: Subjects had a mean (SD) age of 43.8 (13.0), SLE duration of 11.6 (10.4) years, 38% were postmenopausal, 13% had prior non-OP fractures, and 41% used corticosteroids for>3 months. OP and LBM were diagnosed in 14.6% and 8.8% respectively. Significant negative correlations existed between f-neck (r=-0.31, p=0.001) and hip BMD (r=-0.41, p<0.01) with corticosteroid duration. The mean FRAX-Major was 10.2% (6.3) and FRAX-Hip was 1.9% (3.3). FRAX-Major>20% was seen in 12 patients (7 treated). FRAX-Hip>3% was seen in 27 (18 treated). Treatment was given to 19.4% and 14.6% with FRAX-Major<10% and FRAX-Hip<1% respectively. FRAX-Major correlated significantly with: corticosteroid duration (r=0.33, p=0.008) and age (r=0.21, p=0.01). FRAX-Hip correlated significantly with: corticosteroid duration (r=0.35, p=0.03), age (r=0.23, p=0.02), and SLE duration (r=0.20, p=0.01). The mean BR was 9.5 (2.2). BR>10% was in 43.2%. BR significantly correlated with: FRAX-Major (r=0.538, p<0.01), FRAX-Hip (r=0.599, p<0.01), age (r=0.232, p=0.037), SLE duration (r=0.435, p<0.01), and corticosteroid duration (r=0.285, p=0.026). SM and SLE/OP factors had no associations. Conclusion: OP and LBM are prevalent in SLE women. FRAX and HSA provide insight to fracture risk by deriving probabilities for prescribing treatment or assessing bone structure non-invasively. SLE FEMALES IN HIPP STUDY (n= 271) FEMALES > 50 (n=89) FEMALES < 50 (n=182) LOW BONE MASSz-score < -2.0 (n=16) OSTEOPOROSIS t-score < -2.5 (n=13) Figure 1.0: Prevalence calculation stratified according to age • Age • Sex • BMI • Prior fracture (Y/N) • Fracture Family history (Y/N) • Smoking (Y/N) • Corticosteroids (Y/N) • Rheumatoid Arthritis • Secondary OP • Alcohol BACKGROUND Figure 2.0: FRAX Questionnaire • Osteoporosis (OP) is a significant cause of morbidity for women with long-term complications of SLE, with an estimated prevalence ranging from 4%-23%. • Both treatment-related and disease-related factors of SLE are implicated in patients’ susceptibility to OP. Lee, et al. Rheum Dis Clin North Am 2005; 31(2):363-385. • Approximately 60-80% of the bone strength is accounted by BMD, while 20-40% of the strength is dependent on bone quality. Lee, et al. Rheum Dis Clin North Am 2005; 31(2):363-385. • The Fracture Risk Assessment Tool (FRAX) and Hip Structural Analysis (HSA) are new tools used to assess fracture risk. Unnanuntana A, et al. Bone and Joint Surgery 2010; 92:743-753. (NN) (IT) OBJECTIVES (S) In women with SLE, to determine the: • Osteoporosis (OP) and low bone mass (LBM) prevalence in women aged >50 years and <50 years, respectively • Fracture risk using the Canadian Fracture Risk Assessment Tool (FRAX) in women >40 years • Bone quality by Hip Structural Analysis (HSA) • Correlations between FRAX and HSA with SLE/OP risk factors. Fracture Risk Assessment and Hip Structural Analysis in Canadian Females Living with Systemic Lupus Erythematosus (SLE) JJ. Lee, AM. Cheung, E. Aghdassi, S. Morrison, V. Peeva, C. Neville, S. Hewitt, D. Da Costa, J. Pope, PR. Fortin. Division of Rheumatology, The University Health Network, Toronto, Canada, McGill University, Montreal, UWO, London ON. TABLE 4: FRAX SCORES IN SLE FEMALES >40 Statistical Analysis: • Descriptive summary statistics as Mean±SD or as Percentage • Un-paired student’s t-test for two groups’ comparison • Pearson correlations for associations between FRAX, HSA, and SLE/OP factors RESULTS • Out of 12 with FRAX-Major >20%, 7 were on OP meds • Out of 27 with FRAX-Hip >3%, 18 were on OP meds • Unnecessary OP meds given to 22% according to FRAX-Major • Unnecessary OP meds given to 16.7% according to FRAX-Hip TABLE 1: DEMOGRAPHIC CHARACTERISTICS • Body Mass Index • Menopause status • Smoking Status • Alcohol • Prior non-OP fractures • Family history of OP TABLE 5: HSA IN A SUBSET OF FEMALES (n=81) • BR >10% at the NN was seen in 43.2% (n=35) (10.01 – 14.83) ASSOCIATIONS OF BMD VALUES WITH SLE/OP RISK FACTORS • F-neck BMD was significantly correlated with corticosteroid duration (r=-0.31, p=0.001) • Total Hip BMD was significantly correlated with: corticosteroid duration (r=-0.41, p<0.01) ASSOCIATIONS OF FRAX SCORES WITH SLE/OP RISK FACTORS • FRAX-Hip was significantly correlated with: corticosteroid duration (r=0.35, p=0.005), Age (r=0.23, p=0.02), SLE duration (r=0.20, p=0.01) • FRAX-Major was significantly correlated with: corticosteroid duration (r=0.33, p=0.008) and Age (r=0.21, p=0.01) ASSOCIATIONS OF HSA WITH SLE/OP/FRAX RISK FACTORS • BR at the NN was significantly correlated with: FRAX-Major (r=0.54, p<0.01), FRAX-Hip (r=0.60, p<0.01), Age (r=0.23, p=0.04), SLE duration (r=0.43, p<0.01), corticosteroid duration (r=0.28, p=0.03) • There were no significant correlations of SM at NN with risk factors Fracture Risk Assessment Tool (FRAX): • Fracture probability was calculated in SLE patients >40 using the Canadian population (version 3.2). http://www.sheffield.ac.uk/FRAX • Questionnaire: Femoral neck BMD + clinical risk factors: • Results: FRAX-Major: Probability of major osteoporotic event in 10 years FRAX-Hip: Probability of hip fracture event in 10 years • Interpretation: FRAX-Major >20% are at high risk and need OP treatment FRAX-Hip >3% are at high risk and need OP treatment TABLE 2: BONE MINERAL DENSITY AND PREVALENCE OF OSTEOPOROSIS IN FEMALES >50 DISCUSSION • Study showed OP prevalence of 14% in those >50 and a LBM prevalence of 8.8% in <50 . Prevalence values may be an underestimate because of our exclusion criteria. • In those >40, 7-15.8% were at risk for major/hip fractures using FRAX. FRAX-Major values were not found to be significantly correlated with SLE duration. FRAX may underestimate fracture risk in SLE females. • BR values were positively correlated with OP/SLE risk factors. SM values were negatively correlated with these risk factors. SM and BR values were in similar range to other HSA studies. • To our knowledge, this is the first study that reports LBM prevalence in SLE patients by grouping according to age and using z-scores, and to report FRAX and HSA values in SLE females. Hip Structural Analysis (HSA): • Structural dimensions at the left femur • 3 regions: NN, IT, S were assessed through DEXA scans • Results: Section Modulus (SM): Index of bending loads Buckling Ratio (BR): Estimate of cortical stability and susceptibility to buckling under loads • Interpretation: SM decreases fracture risk, BR increases fracture risk BR >10% is considered high fracture risk TABLE 3: BONE MINERAL DENSITY AND PREVALENCE OF LOW BONE MASS IN FEMALES <50 Figure 3.0 HSA assessment of structural dimensions The study was funded by the Canadian Institute for Health Research and The Arthritis Society