Download
1 / 21
480 likes | 3.78k Vues
SCAPULAR DYSKINESIS & ITS RELATION TO SHOULDER PAIN. W.Kibler , John McMullen J Am Acad Orthop Surg 2003 A JOURNAL ARTICLE REVIEW . ARTICLE INCLUDES. Normal scapular function Scapular Dyskinesis Methods of classification Evaluation techniques. SCAPULAR DYSKINESIS.

E N D
SCAPULAR DYSKINESIS & ITS RELATION TO SHOULDER PAIN W.Kibler , John McMullen J Am Acad Orthop Surg 2003 A JOURNAL ARTICLE REVIEW
ARTICLE INCLUDES • Normal scapular function • Scapular Dyskinesis • Methods of classification • Evaluation techniques
SCAPULAR DYSKINESIS • It is defined as observable alterations in the position of the scapula & the patterns of scapular motion in relation to thoracic cage • The term does not suggest etiology or define patterns that correlate with specific shoulder injuries • Classification of scapular dyskinesis patterns and positions can help to determine treatment • Factors responsible Bony posture or injury contractures & other flexibility problems Alteration in muscle function
SCAPULAR EVALUATION SHOULD INCLUDE • Postural evaluation • Resting Scapular Evaluation • Dynamic Evaluation of scapular motion • Corrective measures
STATIC EVALUATION SCAPULAR EVAL SHOULD BE DONE FROM POSTERIOR ASPECT FIRSTLY SCAPULA SHOULD BE EVALUATED IN STATIC POSITION AS IN LONG-STANDING SCAPULAR DYSKINESIS,RESTING WINGING MAY BE SEEN
DYNAMIC EVALUATION • Should be examined in both elevating & lowering phase of motion • Muscle weakness & mild dyskinesis is commonly seen in lowering phase of arm movement • These commonly present as hitch or jump in otherwise smooth motion of scapula and may be more noticeable with several repetitions
TYPE I PROMINENCE OF INFERIOR MEDIAL SCAPULAR BORDER ABNORMAL ROTATION AROUND TRANSVERSE AXIS INDICATES WEAKNESS OF LOWER TRAP, LAT DORSI, SERR ANT OR TIGHT PECT MINOR,MAJOR
TYPE II CLASSIC WINGING PROMINENCE OF ENTIRE MEDIAL SCAPULAR BORDER ABNORMALROTATION AROUND VERTICAL AXIS INDICATES WEAKNESS OF SERR ANT,RHOMBOIDS,ALL FIBERS OF TRAP
TYPE III PROMINENCE OF SUPERIOR MEDIAL SCAPULAR BORDER WITH SUPEROR TRANSLATION OF ENTIRE SCAPULA INDICATES OVERACTIVITY OF LEVATOR SCAPULAE & IMBALANCE OF UPPER & LOWER TRAP FORCE COUPLE
TESTS PERFORMED TO INDICATE WEAKNESS OF SCAPULAR MUSCLES • Isometric scapular pinch test • Wall push- ups • Lateral scapular slide test • Scapular assistance test • Scapular retraction test
ISOMETRIC SCAPULAR PINCH TEST • Scapula can be normally held in retraction with isometric pinch for 15 to20 seconds without burning pain or muscle weakness • Scapular ms weakness may manifest as burning pain in less than 15 sec.
WALL PUSH - UPS • Wall push ups are effective for evaluating serratus anterior strength • Abnormalities may be noted with 5 to 10 Wall push –ups
LATERAL SCAPULAR SLIDE TEST • Inferior – medial angle of scapula is palpated & marked on both the sides • The reference point on the spine is nearest spinous process,which is marked • Distance is measured on both the sides in three different positions,- • At resting position • With hands on hips, with fingers anterior &thumb posterior • With the arms at 90 degrees with internal rotation • A 1.5 cm asymmetry is the threshold for abnormality
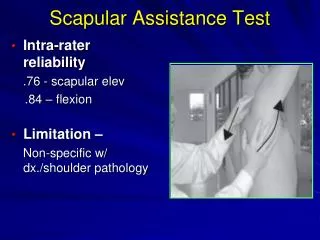
SCAPULAR ASSISTANCE TEST • During abduction or forward elevation, assistance is provided by manually stabilizing the scapula and rotating inferior border of scapula as the arm moves • This proc simulates force couple activity of serratus ant and lower trap • Elimination or modification of symptoms indicate these muscles should be major focus in rehab.
SCAPULAR RETRACTION TEST • The examiner stabilizes the medial scapular border as the arm is elevated or externally rotated. • Relief of impingement symptoms is a positive test
Guidelines for Integrated Rehabilitation of Scapular Dyskinesis Exercises Weeks (estimate) Scapular Motion Thoracic posture 1-3 Trunk flexion/extension/rotation 1-3 Lower abdominal/hip extensor 1-5 Muscular Flexibility Massage 1, 2 Modalities (eg, ultrasound, electronic stimulation) 1-3 Stretching (eg, active-assisted, passive, PNF) 1-8 Corner stretches (pectoralis minor) 1-3 Towel roll stretches (pectoralis minor) 1-3 Levator scapulae stretches 1-3 “Sleeper” position stretches (shoulder ER) 1-3
Closed Kinetic Chain Co-contraction Exercises Weight-shifting 1, 2 Balance board 1, 2 Scapular clock 1, 2 Rhythmic ball stabilization 2 Weight-bearing isometric extension 1, 2 Wall push-up 2 Table push-up 3-5 Modified to prone push-up 5-8 Axially Loaded AROM Exercise Scaption slide 2-5 Flexion slide 2-5 Abduction glide 3-5 Diagonal slides 2-6
Integrated Open Kinetic Chain Exercises Scapular motion exercices plus arm elevation 3-8 Unilateral/bilateral tubing pulls with trunk motion 4-8 Modified lawn mower series 3-6 Dumbbell punches with stride (progressive height and resistance) 6-8 Lunge series with dumbbell reaches 5-8 Plyometric Sport-Specific Exercises Medicine ball toss and catch 6-10 Reciprocal tubing plyometrics 6-10
THANK YOU PRESENTATION ACKNOWLEDGEMENT: DR. PALLAVI SHIVALKAR ASSOCIATE PROFESSOR, DR. D .Y PATIL COLLGE OF PHYSIOTHERAPY NERUL, NAVI MUMBAI THANK YOU MADAM……. DR. AJIN JAYAN THOMAS