Download
1 / 65
650 likes | 1.17k Vues
A very sick neonate with pancytopenia, profound hypocalcemia and extreme hyperphosphatemia. Dr. CO Sham and Dr. K Tse (Cons., TMH) Prepared on July 2011. History.

E N D
A very sick neonate with pancytopenia, profound hypocalcemia and extreme hyperphosphatemia Dr. CO Sham and Dr. K Tse (Cons., TMH) Prepared on July 2011
History • Maturity 37 week and 5 days, birth weight 2.5 kg, delivered by Caesarean Section at St. Teresa Hospital because of maternal preference • Both parents had known alpha thalassaemia trait, Mother alpha thal 1; Father alpha thal 2 Quong Sze (native city 'Kai-ping') • Parents unrelated. • Mother also had chronic hepatitis B.
History • Previous child died at Tuen Mun Hospital in April 2008 on second day of life because of meconium aspiration, pulmonary hypertension of newborn and Hb H disease. • Antenatal course of the current pregnancy was uneventful. Followed up both at O&G, Tuen Mun Hospital and private O&G doctor. • Baby was well after delivery. • Hepatitis B vaccine and HBIG were given shortly after delivery, and BCG given over left shoulder on 16-4-2011. • Baby was FU daily by a private Pediatrician in first 7 days of life. Told to be normal all along. A strong odour was noted since birth by the family, but the parents were told that it was normal.
Current admission • Admitted via A&E, TMH on Day 14 of life at 1:24 am because of cough, shortness of breath and poor feeding for 1 day • No fever all along • Decreased feeding from 30 ml X 6 per day down to 15 ml X 4 in 1 day • Decreased urine output and no bowel opening for 1 day • Seen by a private doctor at Tuen Mun, given ibuprofen, infacol, piriton, U-Eaton, domperidone and pro-amine, but the condition did not improve. Therefore, the parents brought the child to A&E • No sick family members • No recent travel outside Hong Kong
Physical examination • Tired looking with fair general condition • Capillary refill 2 seconds • Dry oral mucosa with normal skin turgor • BW 2.42 kg (birth wt 2.5 kg), BH 47 cm, HC 34 cm • Respiratory rate 50/min; Apical rate 140/min • Axillary temperature 36.4∘C
Physical examination • Left shoulder: normal looking, and BCG scar not seen • Chest: subcostal insucking with decreased air entry over right middle zone • CVS: normal heart sound, no murmur • Abdomen: soft and distended, liver 2 cm below costal margin, no splenomegaly, bowel sound active • CNS: AFNT • Skin: no rash
Maternal grandmother 58-year-old Paternal grandmother 56-year-old Maternal grandfather 66-year-old Paternal grandfather 58-year-old Father 31-year-old Mother 30-year-old Maternal uncle 35-year-old Maternal uncle 34-year-old Paternal uncle 30-year-old Died on 2nd day of life in 2008 because of pulmonary hypertension of newborn and Hb H disease. Miscarriage at 9th week gestation in May 2010 Our patient Family tree
Progress • Sepsis work up performed including blood culture, lumbar puncture and bladder catheterization • First venous blood gas: pH 7.30, pCO2 3.5, pO2 5.1, BE -12.2 • 2 boluses of normal saline 10 ml/kg given • Started on ampicillin, and cefotaxime, which was later switched to meropenem • Also started ranitidine in view of brownish substance aspirated from Ryle's tube
Deterioration • At 8:50 am on the same day, in view of increase oxygen requirement, pallor, and septic looking baby with neutropenia, severe hypocalcaemia, hyperphosphataemia, acute renal failure and decompensated metabolic acidosis, baby was transferred to NICU for further care. • Convulsion at 10:00 am at NICU, presented as staring eyes and tonic contraction of 4 limbs. Attack lasted for 30 minutes, stopped by phenobarbitone and bolus of calcium gluconate. • ECG monitoring once showed ectopic beats, but not found on ECG long lead II after calcium supplement given
Acute stage • Double lumen PICC was set via the right long saphenous system • Later the baby was intubated and put on mechanical ventilation for poor respiratory effort • Active bleeding was found from endotracheal tube and Ryle's tube • Repeated transfusions of platelet concentrate, fresh frozen plasma, and vitamin K to stop bleeding. Given pack cells to top up hemoglobin. • Calcium supplement was given, and hyper-phosphataemia improved with hyperhydration
In the middle of the night • Baby dull looking and no response to pain • No sedation all along • Glasgow Coma Scale 3/15 (E1V1M1) • ? Fixed and dilated pupil • Limb hypotonic but reflexes present • Gag reflex present but hyporeflexic • Urgent CT brain arranged
CT brain After baby's condition improved, subsequent CT brain revealed diffuse cerebellar hemorrhage. Seen by neurosurgeon – baby unlikely to benefit from clot evacuation.
Next morning • Baby still in “comatose” state • No response to voice and pain • Pupils equal but sluggish response to light • Nurse reported foul smell inside the incubator • Cerebrospinal fluid and catheterized urine cell counts, and biochemistry indicated that infection was not likely
Stop and think! • Previous baby died of thalassaemia and PPHN • We are now facing a baby with: • ‘Good past health’ Day 14 baby • Severe metabolic acidosis • Pancytopenia • Severe hypocalcaemia and hyperphosphataemia • Foul smelling odour • Cerebellar hemorrhage • No response to pain and voice
Differential diagnosis • Severe infection • Pyogenic infection • Viral infection (HBV, HPV) • Disseminated BCG infection in immuno-compromised host • Tumor lysis syndrome • Inborn error of metabolism • Congenital heart diseases
Help from colleagues of other disciplines • Seen by microbiologist, suspect disseminated herpes simplex infection in view of pneumonia, pancytopenia and derange liver function • Mother had a cold sore over her upper lip • Started on IV acyclovir • (Virus study turned out to be negative) • Blast cells not detected x 2 in P’ smear
Urine organic acid profile • Significant hyper-excretions of isovaleryl-glycine and 3-hydroxy-isovaleric acid and presence of 4-hydroxyisovaleric acid, methylsuccinic acid and mesaconic acid were detected. • The pattern is diagnostic of isovaleric acidemia.
Isovaleric acidemia (異戊酸血症) in the East Asia • At least 7 cases in Taiwan • No new cases after newborn screening for metabolic diseases • Autosomal recessive inheritance • Antenatal screening can be offered http://www.genes-at-taiwan.com.tw/genehelp/database/disease/IVA_940830.htm
Treatment • Started on L-carnitine and L-glycine once diagnosis was confirmed. • Glasgow Coma Scale improved gradually • Started on parenteral nutrition with low levels of amino acids. Later switched to protein free formula. • Gradual step up amount of protein in diet • Monitor ammonia (daily) and carnitine levels
Treatment • Train up oral feeding • Serial USG brain revealed hematoma resolved gradually • Neuro-developmental training offered • Follow up to monitor development • Antenatal counseling to parents for next pregnancy (alpha thalassaemia and isovaleric acidemia)
Future follow up plan • Educate parents and medical team about the presentation of metabolic decompensation • Symptoms and signs: • Ill looking child • Fever • Sweaty feet odour • Recurrent vomiting, diarrhea, severe dehydration • Tachypnoea • Hypothermia • Listlessness, lethargy, seizures and coma • Stroke manifestations, encephalopathy
Stress that may trigger the problem • Increased protein / leucine (rice with high leucine content) intake • Poor diet compliance • Fever and acute infections • Gastroenteritis • Pancreatitis • Vaccinations • Episodes of increased catabolism • Prolonged fasting • Surgical and dental procedures • Trauma (severe) • Strenuous exercise training • Graves’ disease
Counseling & referrals • Counseling by management team, chemical pathologist, then dietician • Written information was given to parents(異戊酸血症) • The sick day plan • Letters to concerning GPs • CMS entries, reminders, drug alerts • Special nurses / ward for further admission • Dietician, speech therapist, physiotherapist and occupational therapist • Child Assessment Center, Eye clinic • Financial problem, the special formula, IVA anamix infant, is very expensive (> $600 / can for long-termed use)
Further points for discussion • Lab monitoring • Misleading presentations • Remove the toxic metabolites • Emergency Tx and cautions • Problems on long-termed FU • Diets • Patient group
Misleading presentations in neonates • Premature infant (32 wk) might have normal serum ammonia level during attack • Sepsis in neonate (E coli) (stop and think even with +ve culture) • Recurrent / severevomiting (leading to pyloromyotomy) (vomiting not improved) • Feeding difficulty, diarrhea, severe dehydration, wt loss, tachypnea, hypothermia, cholestasis, abnormal posturing and movement, spasm, listlessness, • Lethargy, seizures, coma, stroke manifestations, encephalopathy, leading todeath / severe brain damage within a few days if not treated promptly. • Isomil with lower leucine(may present later) • High index of suspicion – characteristic smell of ‘sweat feet’, keto-acidosis, large anion gap, high serum ammonia levels (premature baby?) (dry blood spot test can show the metabolic defect)
Presentations in late onset cases • FTT, selective refusal of protein-rich foods, periodic vomiting, alopecia • ‘Dirty sock’ / unwashed body’ / ‘sweaty feet’ odor +/- smells of ketones in breath during attacks • Abnormal behavior / ‘psychosomatic’ attacks after meal / in afternoon (rather than in the morning) • Learning difficulties, isolated cognitive impairment, developmental delay, mental retardation, needs of special school. • Movement disorders (tremors, choreoathetosis, dystonia), seizures, generalized hypotonia, intermittent ataxia, repeated acute episodes, abnormal postures / movements / behavior • Dizziness and blurred vision and unsteady gait in teenager; • Constipation, abdominal distension / pain, pancreatitis. • Fanconi syndrome, proximal RTA, hyperchloremic metabolic acidosis. • Secondary carnitine def. as heart failure, conduction disturbances, sensitivity to other potentially cardiotoxic medications. • Dwarfism, cataract and congenital abnormalities. • Some may attend normal school, attending college / university, +/- independent life.
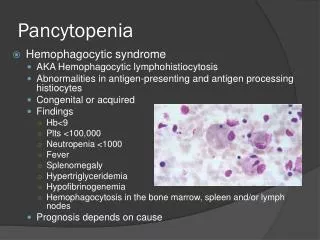
Other misleading presentations • Late onset cases may have huge hyperammonaemia (200 – 1400 μM), without ketoacidosis, mistaken as urea cycle disorder • Leukothrombocytopenia +/- anemia / pancytopenia / extra-medullary hematopoiesis, resembling promyelocytic leukemia, (no blast cells in [repeated] peripheral smear, 15:17 translocation not present), arrest of myeloid series at the promyelocytic stage, isovaleric acid is toxic to bone marrow • Hyperglycemia(mistaken as DKA, but very sensitive to insulin, normal Hb A1c, repeated episodes) • Stoke manifestations, intra-cranial / ventricular / cerebral / cerebellar bleeding, +/- brain imaging for attacks (think of metabolic causes) • Acute / chronic / hemorrhagic pancreatitis, Dx by raised amylase +/- imaging, known Cx, also in relapses (causes?) • Strenuous exercise training (offensive body / sweaty feet odor!? Large anion gap metabolic acidosis Vs heat stroke!?) • Mild phenotype / asymptomatic IVA (932C>T) (A282V) detected by neonatal screening
Misleading presentations in ‘already known’ cases • Use of pivalate-generating drugs / antibiotics (adefovir dipivoxil, cefteram / cefditoren / cefetamet pivoxil, and pivamicillin, in general NA in TMH, except adefovir) may affect the cutoff value of C5 acyl-carnitine, please interpret the results with chemist / chemical pathologist & check the drugs with pharmacist • Some pt may withhold Tx thinking that they have been ‘cured’, not telling others / doctors on their previous events, then comatose sometimes later.(Entry to CMS, reminder, drug alert; written / repeated warning to parents & patient) • Graves’ disease (attack in stably treated IVA case, to Dx Graves’ Ds!?)
Laboratory findings in acute decompensation stage Leukothrombocytopenia, anemia, (pancytopenia) Ketouria Acidosis with large anion gap Hypocalcemia, hyperphosphataemia (severely reduced ratio of phosphocreatine to inorganic phosphate, indicating a major impairment of oxidative phosphorylation), hypomagnesaemia Hypo-/hyperglycemia (mistaken as diabeteic ketoacidosis) Hyperammonaemia Raised amylase (pancreatitis) Hyperlactacidemia, hyperuricemia, abnormal LFT, hypoalbuminemia, hyperargininemia. Intra-cranial (cerebral / cerebellar) bleeding To check CBC, Astrup, ketone bodies, ammonia, amylase, lactate, dried blood spot test, L/RFT, Ca, PO4, Mg, PT, APTT +/- imaging
Remove the toxin • High dose (IV, but NA in HA!?)carnitine (100-400 mg/kg/day) in 3-4 divided doses, (oral 1 g tds) • Oral glycine (250-800 mg/kg/day) in 2-4 divided doses (glycine 200 mg/kg every 6 hr can be given rectally if oral intolerance) (also rectal carnitine?) • Consider dialysis or haemofiltration if for ammonia > 400 – 600μmol/l • Oral carbamyl-glutamate 50 mg/kg/day in 4 divided doses may also help to reduce the ammonia level. • Fluid restriction if cerebral edema • Target at no / low leucine metabolites, and normal serum ammonia levels) (plasma leucine peak 2 hr after leucine loading).
Dialysis!? • For ammonia > 400μmol/l, or persistent > 8 hr • PD / extracorporeal dialysis / continuous hemo-filtration / hemodialysis [Tx of choice] • Good outcome with pre-dialysis coma duration < 33 hr in neonates, rather than initial blood ammonium / leucine levels • Cx – severe hypotension / circulatory failure, ischemia of limb after cannulation of femoral vessels, pulmonary / pericardial hemorrhage, thrombosis, sepsis, rebound, failure to decrease ammonium level). • Oral N-carbamyl-glutamate (carglumic acid)(NA in HA, not registered in HA, unregistered drug? HK$ 1,083 / 200 mg tablet, a single purchase at least 60 tablets, i.e., HK$ 65,000) (more recent information: another vender, $1,300 / 200 mg tablet, single purchase of 5 tablets, i.e., $6,500, for N-acetylgutamate synthetase def. initial dose 100-200 mg/kg/d, maintenance dose 10-100 mg/kg/d)50-150 mg/kg/d (up to 250 mg/kg/d) in 4 divided doses can help to reduce the ammonia level, without / avoiding dialysis.
Oral drug to reduce serum ammonium? • Oral N-carbamyl-glutamate (carglumic acid) 50-150 mg/kg/d (up to 250 mg/kg/d) in 4 divided doses may also help to reduce the ammonia level (effectively used orally in term infant reported) (SE – 13%, vomiting, abdominal pain, pyrexia, tonsillitis, anemia, ear infection, diarrhea, nasopharyngitis, and headache) • Use of sodium benzoate to increase ammonia detoxication is controversial, benzoic acid with its CoA metabolite competing with isovaleryl-CoA for glycine N-acylase, preventing the beneficial effect of glycine.
Medical emergency – Tx Fluid and rehydration Correct electrolyte disturbance Treat concomitant sepsis, start empirical antibiotic (patient likely neutropenic) Correct bleeding diathesis Inhibition of endogenous catabolism by adequate energy supply, and use of leucine free milk formula +/- low dose parenteral nutrition