Download
1 / 39
400 likes | 541 Vues
Chapter 23: The Elbow. Anatomy of the Elbow. Functional Anatomy. Complex that allows for flexion, extension, pronation and supination 145 degrees of flexion and 90 degrees of supination and pronation

E N D
Functional Anatomy • Complex that allows for flexion, extension, pronation and supination • 145 degrees of flexion and 90 degrees of supination and pronation • Bony limitations, ligamentous support and muscular stability at the elbow help to protect it from overuse and traumatic injuries • Elbow demonstrates a carrying angle due to distal projection of humerus • Normal in females is 10-15 degrees, males 5 degrees • Critical link in kinetic chain of upper extremity
Assessment of the Elbow • History • Past history • Mechanism of injury • When and where does it hurt? • Motions that increase or decrease pain • Type of, quality of, duration of, pain? • Sounds or feelings? • How long were you disabled? • Swelling? • Previous treatments?
Observations • Deformities and swelling? • Carrying angle • Cubitus valgus versus cubitus varus • Flexion and extension • Cubitus recurvatum • Elbow at 45 degrees • Isosceles triangle (olecranon and epicondyles)
Humerus Medial and lateral epicondyles Olecranon process Radial head Radius Ulna Medial and lateral collateral ligaments Annular ligament Biceps brachii Brachialis Brachioradialis Pronator teres Triceps Supinator Wrist flexors and extensors Palpation: Bony and Soft Tissue
Special Tests • Circulatory and Neurological Function • Pulse should be taken at brachial artery and radial artery • Skin sensation should be checked - determine presence of nerve root compression or irritation in cervical or shoulder region • Tinel’s sign • Ulnar nerve test • Tap on ulnar nerve (in ulnar groove) • Positive test is found when athlete complains of sensation along the forearm and hand • Test for Capsular Injury • Tested after hyperextension of elbow • Elbow is flexed to 45 degrees, wrist is fully flexed and extended • If joint pain is severe, moderate/severe sprain or fracture should be suspected
Valgus/Varus Stress Test • Assess injury to the medial and lateral collateral ligaments, respectively • Looking for gapping or complaint of pain
Medial and Lateral Epicondylitis Tests • Elbow flexed to 45 degrees and wrist extension or flexion is resisted • Pain at lateral or medial epicondyle, respectively indicates a positive test • Pinch Grip Test • Pinch thumb and index finger together • Inability to touch fingers together indicates entrapment of anterior interosseous nerve between heads of pronator muscle • Pronator Teres Syndrome Test • Forearm pronation is resisted • Increased pain proximally over pronator teres indicates a positive test
Functional Evaluation • Pain and weakness are evaluated through AROM, PROM and RROM • Flexion, extension, pronation and supination • ROM of pronation and supination are particularly noted
Recognition and Management of Injuries to the Elbow • Subject to injury due to broad range of motion, weak lateral bone structure, and relative exposure to soft tissue damage • Many sports place excessive stress on joint • Locking motion of some activities, use of implements, and involvement in throwing motion make elbow extremely susceptible
Contusion • Etiology • Vulnerable area due to lack of padding • Result of direct blow or repetitive blows • Signs and Symptoms • Swelling (rapidly after irritation of bursa or synovial membrane) • Management • Treat w/ RICE immediately for at least 24 hours • If severe, refer for X-ray to determine presence of fracture
Olecranon Bursitis • Etiology • Superficial location makes it extremely susceptible to injury (acute or chronic) --direct blow • Signs and Symptoms • Pain, swelling, and point tenderness • Swelling will appear almost spontaneously and w/out usual pain and heat • Management • In acute conditions, compression for at least 1 hour • Chronic cases require superficial therapy primarily involving compression • If swelling fails to resolve, aspiration may be necessary • Can be padded in order to return to competition
Strains • Etiology • MOI is excessive resistive motion (falling on outstretched arm), repeated microtears that cause chronic injury • Rupture of distal biceps is most common muscle rupture of the upper extremity • Signs and Symptoms • Active or resistive motion produces pain; point tenderness in muscle, tendon, or lower part of muscle belly • Management • RICE and sling in severe cases • Follow-up w/ cryotherapy, ultrasound and exercise • If severe loss of function encountered - should be referred for X-ray (rule out avulsion or epiphyseal fx
Ulnar Collateral Ligament Injuries • Etiology • Injured as the result of a valgus force from repetitive trauma • Can also result in ulnar nerve inflammation, or wrist flexor tendinitis; overuse flexor/pronator strain, ligamentous sprains; elbow flexion contractures or increased instability • Signs and Symptoms • Pain along medial aspect of elbow; tenderness over MCL • Associated paresthesia, positive Tinel’s sign • Pain w/ valgus stress test at 20 degrees; possible end-point laxity • X-ray may show hypertrophy of humeral condyle, posteromedial aspect of olecranon, marginal osteophytes; calcification w/in MCL; loose bodies in posterior compartment
Ulnar Collateral Ligament Injuries (cont.) • Management • Conservative treatment begins w/ RICE and NSAID’s • W/ resolution, strengthening should be performed; analysis of the throwing motion (if applicable) • Surgical intervention may be necessary (Tommy John procedure) • Throwing athlete can return to activity 22-26 weeks post surgery
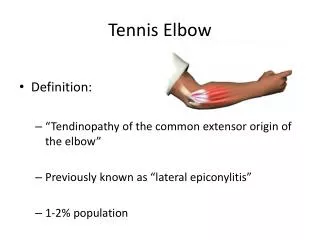
Lateral Epicondylitis (Tennis Elbow) • Etiology • Repetitive microtrauma to insertion of extensor muscles of lateral epicondyle • Signs and Symptoms • Aching pain in region of lateral epicondyle after activity • Pain worsens and weakness in wrist and hand develop • Elbow has decreased ROM; pain w/ resistive wrist extension
Lateral Epicondylitis (continued) • Management • RICE, NSAID’s and analgesics • ROM exercises and PRE, deep friction massage, hand grasping while in supination, avoidance of pronation motions • Mobilization and stretching in pain free ranges • Use of a counter force or neoprene sleeve • Mechanics training
Medial Epicondylitis • Etiology • Repeated forceful flexion of wrist and extreme valgus torque of elbow • Signs and Symptoms • Pain produced w/ forceful flexion or extension • Point tenderness and mild swelling • Passive movement of wrist seldom elicits pain, but active movement does • Management • Sling, rest, cryotherapy or heat through ultrasound • Analgesic and NSAID's • Curvilinear brace below elbow to reduce elbow stressing • Severe cases may require splinting and complete rest for 7-10 days
Elbow Osteochondritis Dissecans • Etiology • Impairment of blood supply to anterior surface resulting in degeneration of articular cartilage, creating loose bodies • Repetitive microtrauma in movements of elbow rotation, extension, valgus stress causing compression of the radial head ad shearing of the radiocapitular joint • Seen in young athletes involved in throwing motion • Panner’s disease in incidents of children age <10 • Signs and Symptoms • Sudden pain, locking; range usually returns in a few days
Signs and Symptoms (continued) • Swelling, pain at radiohumeral joint, creptitus, decreased ROM (full extension); grating w/ pronation and supination • X-ray may show flattening and crater of capitulum w/ loose bodies • Management • Activity restriction for 6-12 weeks; NSAID’s • Splint and cast applied for cases of extensive deterioration • If repeated locking occurs, loose bodies are removed surgically
Little League Elbow • Etiology • Caused by repetitive microtraumas that occur from throwing (not type of pitch) • May result in numerous disorders of growth in the pitching elbow • Signs and Symptoms • Onset is slow; slight flexion contracture, including tight anterior joint capsule and weakness in triceps • Athlete may complain of locking or catching sensation • Decreased ROM or forearm pronation and supination
Little League Elbow (continued) • Management • RICE, NSAID’s and analgesics • Throwing stops until pain resolved and full ROM is regained • Gentle stretching and triceps strengthening • Throwing under supervision w/ good technique to prevent recurrence
Cubital Tunnel Syndrome • Etiology • Pronounced cubital valgus may cause deep friction problem • Ulnar nerve dislocation • Traction injury from valgus force, irregularities w/ tunnel, subluxation of ulnar nerve due to lax impingement, or progressive compression of ligament on the nerve • Signs and Symptoms • Pain medially which may be referred proximally or distally • Tenderness in cubital tunnel on palpation and hyperflexion • Intermittent paresthesia in 4th and 5th fingers
Cubital Tunnel Syndrome (continued) • Management • Rest, immobilization for 2 weeks w/ NSAID’s • Splinting or surgical decompression or transposition of subluxating nerve may be necessary • Athlete must avoid hyperflexion and valgus stresses
Dislocation of the Elbow • Etiology • High incidence in sports caused by fall on outstretched hand w/ elbow extended or severe twist while flexed • Bones can be displaced backward, forward, or laterally • Distinguishable from fracture because lateral and medial epicondyles are normally aligned w/ shaft of humerus • Signs and Symptoms • Swelling, severe pain, disability • Complications w/ median and radial nerves and blood vessels • Often a radial head fracture is involved
Management • Cold and pressure immediately w/ sling • Refer for reduction • Neurological and vascular fxn must be assessed prior to and following reduction • Physician should reduce - immediately • Immobilization following reduction in flexion for 3 weeks • Hand grip and shoulder exercises should be used while immobilized • Following initial healing, heat and passive exercise can be used to regain full ROM • Massage and joint movement that are too strenuous should be avoided before complete healing due to high probability of myositis ossificans • ROM and strengthening should be performed and initiated by athlete (forced stretching should be avoided
Fractures of the Elbow • Etiology • Fall on flexed elbow or from a direct blow • Fracture can occur in any one or more of the bones • Fall on outstretched hand often fractures humerus above condyles or between condyles • Condylar fracture may result in gunstock deformity • Direct blow to ulna or radius may cause radial head fracture as well • Signs and Symptoms • May not result in visual deformity • Hemorrhaging, swelling, muscle spasm
Elbow Fractures (continued) • Management • Decrease ROM, neurovascular status must be monitored • Surgery is used to stabilize adult unstable fracture, followed by early ROM exercises • Stable fractures do not require surgery • Removable splints are used for 6-8 weeks
Volkmann’s Contracture • Etiology • Associate w/ humeral supracondylar fractures, causing muscle spasm, swelling, or bone pressure on brachial artery, inhibiting circulation to forearm • Can become permanent • Signs and Symptoms • Pain in forearm - increased w/ passive extension of fingers • Pain is followed by cessation of brachial and radial pulses, coldness in arm • Decreased motion • Management • Remove elastic wraps or casts • Close monitoring must occur
Rehabilitation of the Elbow • General Body Conditioning • Must maintain pre-injury fitness levels - cardiovascular and strength (lower body) • Flexibility • Restoring ROM is critical in elbow rehab • Variety of approaches can be used as long as they don’t force the joint • Joint Mobilizations • Loss of proper arthrokinematics following immobilization is expected • Joint mobilization and traction can be very useful to increase mobility and decrease pain through restoration of accessory motions
Strengthening • Achieved through low-resistance, high-repetition exercises - must be pain free • Shoulder and grip exercises should also be performed • Continuous passive motion units followed by dynamic splinting is ideal following surgery • Isometrics can be used while elbow is immobilized • PNF and isokinetics are useful in early and intermediate active stages of rehab • A graded PRE program w/ tubing, weights or manual resistance should be included • Closed kinetic chain activities should also be incorporated - assist in both static and dynamic stability to the elbow • Proprioceptive training should also incorporated
Functional Progressions • Will enhance healing and performance • PNF, swimming, pulley machines and rubber tubing • to simulate sports activities • Should include steps • Warm-up • Gradual build up to activity, becoming increasingly more difficult • Return to Activity • Can re-engage in activity when criteria has successfully been completed • ROM w/in normal limits, strength should be equal w/ no complaint of pain • Return should progress with use of restrictions in an effort to objectively measure activity progression
Protective Taping and Bracing • Should be continued until full strength and flexibility have been restored • Chronic conditions usually cause gradual debilitation of surrounding soft tissue • Must restore maximum state of conditioning w/out encouraging post-injury aggravation