Download
1 / 17
170 likes | 271 Vues
Managing Choice & Demand. Linking Access, Booking, Choice, Demand Management and ‘Evercare’. Context. Clinical services strategy Biggest cost pressures: Unscheduled care Tertiary services Reference costs - £1m saving across community services Arbitration.

E N D
Managing Choice & Demand Linking Access, Booking, Choice, Demand Management and ‘Evercare’
Context • Clinical services strategy • Biggest cost pressures: • Unscheduled care • Tertiary services • Reference costs - £1m saving across community services • Arbitration
ABCDE Strategy • Patient Centred approach • Managing demand • Offering Choice – who, where, how • Waiting time management from referral • Adapted Evercare model • Using new opportunities (nGP Contract + new APMS, Primary Care Collaborative)
How • Leatherhead pilot • enhanced CDM, based on Evercare model • maximising use of community hospitals, community teams + assistive technology • PCT referral management centre & booking office • Supports choice at point of referral • Target referrals into 20 more appropriately • Reduce outpatient waiting times • Expert patients – direct self referral? • Cobham DTC (May 2005)
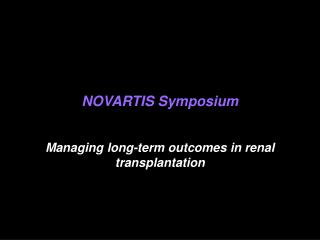
Proposed new system PatientGP GP • Information to practices • Practices refer with current waiting times for all choices available • Changes in referral patterns tracked/use of PCT interface services • reinforced • Detailed comparative analysis to identify issues/trends for review • Provides information on realtime basis - active system of • feedback & information updates to support choice at referral • Creates SAFETY NET - any referrals with “avoidable long waits” • held at RMC and queried back to GP/Practice before releasing • Transmission Issues • RMC records and sends on GP referrals on day of receipt (max delay • for referrals should be only 24 hours) • All non emergency tertiary referrals routed via PCT panel - • max delay for referrals should be 2 weeks • Booking • GP may book appointment (e-booking, fax or letter). OR, • Patient may book appointment later after consulting diary/relatives • etc (telephone). Booking office will contact GP if patient does not • make contact within specified time • Caldicott & Patient Confidentiality • Patient identifiable information is recorded as it will be necessary to • track patients through the referral system / offer them choice • All reports from the RMC database will be non-identifiable • Briefing paper on Caldicott being prepared • Prior to commencement, these issues to be discussed and “signed • off” by PCT Clinical Governance Lead & LMC • Referral Management Centre & Booking Office • Collects & analyses referral info • Feedback to GPs • Triage • Diagnostic tests • Directory of Services • Info template from NPFIT • National & local database • info re service options including • waiting times • Info re take up of choice to PCT • Info re PCT interface services to • challenge referrals to acute Patient offered choice Choice confirmed Patient follow up & discharge Treatment
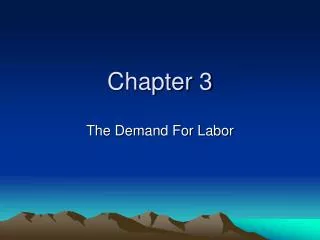
Patient GP Patient Directory of Services Information included Choice offered PCT in GP surgery interface service The system is flexible – either Diagnostic of these options is test and/or also possible Treatment Option 1 Option 2 Option 3 PCT acute acute Choice offered by GPSI/PSI interface service if further treatment required Directory of Services Information included Option 1 Option 2 Option 3 Treatment of patient in PCT interface service or hospital PCT acute acute interface service Patient follow up (if required) Treatment of patient in PCT Discharge interface service or hospital
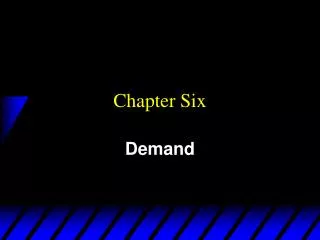
Proposed System PCT Information Choice Web based DoS GP SW London LIS Patient National Guidelines E refer E book RiO/ Booking Office Option 1: Acute Services Option 2: PCT Interface Services Option 3: Acute Services
Proposed GP process Instructions GP Patient Directory of Services Surgery Staff Booking Confirmation Referral Letter BMS RiO Electronic Booking System PCT Back Pain Interface Services
EEMS Directory of ServicesHow is choice offered Types of data held for each service includes: • Service Information – e.g. who, where, what, waiting times. • Clinical Information – e.g. the description of the services being offered and clinical referral guidelines. • Practical Information – e.g. location maps, patient information leaflets, car parking fees, Cobham Booking Office contact details
E-Referral & E-Booking using RiO System Find Clinic Find Appointment Book Appointment
Linking Booking, Choice Demand & Evercare • Using RIO (an existing system) to test e-referrals & e-booking processes for interface services • Developing PCT referral management centre & booking office - go live July • Expanding/flexing flex diagnostic capacity- mobile equipment, PMS specialist for radiology • Expert patients – promoting self management, using collaborative
Using learning from Choice for demand management • Added value of Choice • Patient has an informed debate • Information for patients • Clarity about implications of options • “What and when” to “type of treatment” • Culture change • Step change • Getting used to electronic system • Impact on consultation & practice processes • Bridging infrastructure gap between now and NPfIT