Download
1 / 50
500 likes | 647 Vues
VACCINE S. Immunobiology (Ma rch 10, 2014 ). Objectives:. 1. A brief review of the types of currently used vaccines and the mechanisms of protection; 2. To understand the importance of herd immunity and the relationship between Ro and Po ;

E N D
VACCINES Immunobiology (March 10, 2014)
Objectives: • 1. A brief review of the types of currently used vaccines and the mechanisms of protection; • 2. To understand the importance of herd immunity and the relationship between Ro and Po; • 3. To understand the general requirement for vaccine development; • 4. To understand new approaches, targets and challenges in current vaccine development
I. Herd Immunity and vaccination • An effect whereby vaccination of a large proportion of the population hinders the transmission of an infectious agent and thereby protects the entire population, even those not vaccinated.
Herd Immunity • Immunity in the whole population level. • R0 (basic reproduction number or basic reproductive rate/ratio): the average number of secondary cases produced by one primary case in population with no immunity. • WhenR0 < 1, the infection will die out in the long run. But ifR0 > 1,the infection will be able to spread in a population. • The larger the value of R0, the higher percentage of the population requires vaccination for controlling the disease • P0, proportion of the population that needs to be vaccinated to provide herd immunity and prevent sustained spread of the infection, is given by 1 − 1/R0. • It is not necessary to vaccinate every individual to achieve population protection.
Inverse relationship between vaccination and natural infection
Vaccination rate for some infections • Virtually impossible to reach 100% vaccination
Vaccination • The process of administrating antigen to a live host with the purpose of inducing an immune response for public health reasons
Vaccines • Infectious diseases • Cancer • Allergy and autoimmune diseases • Therapeutic vaccines for chronic infectious diseases and cancers
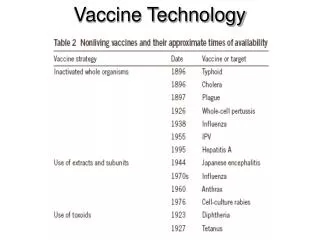
Currently used vaccines (important points) • Subunit (capsular polysaccharide and protein) vs whole cell vaccine; • Live vs killed vaccine • Advantages and disadvantages of live and killed vaccines • Current bacterial and viral vaccines ; • Vaccine are used either on a regular schedule or for special indications
HPV vaccine • Cancer vaccine • prevents infection with certain species of human papillomavirus[HPV types (HPV-16 and HPV-18)] associated with the development of cervical cancer, genital warts(HPV-6,HPV-11), and some less common cancers • Yong women • Male?
Different vaccines are used at different ages Target groups for new vaccines
Advantages/disadvantages of live and killed vaccines Iatrogenic (vaccine-induced) polio
Mechanisms by which current vaccines induce protection • - Polysaccharide vaccines activate B lymphocytes as T cell independent antigens • Conjugated vaccines enhance antibody responses, particularly better for >2 yr old (Hib, Meningitis) • - Protein and killed whole cell vaccines induce B cells to produce antibodies in association with T cell help • - Live vaccines induce cytotoxic T cell responses, inflammatory T cells, and antibodies(mucosal IgA when given by mucosal routes
Primary Requirement of Vaccines • -Safety • -Efficacy • - Seroconversion • - CMI • - Protection (animal, clinical trial)
Stages of Clinical Trials to Establish Safety and Efficacy • -Phase I: to test safety, if possible test immune response; • -Phase II: challenge infection( small scale); Detailed immunological study • -Phase III: vaccinate large population in endemic area (more vaccine come to phase III without challenge infection, phase ii)
THE General IMMUNOLOGICAL REQUIREMENTS FOR SUCCESSFUL VACCINATION • Activation or infection of APCs so that antigens are processed and antigenic peptides are presented in association with class I/II MHC. • Activation of both T and B cells to give a high yield of memory cells (High quality memory T cells). • Generation of Th and cytotoxic T cells which recognize a variety of determinants, in order to overcome potential variation in MHC polymorphism. • Persistence of foreign antigen in its native conformation on follicular dendritic cells in lymphoid tissue, where B memory cells are formed and “recruited over time by the persisting antigen to form antibody secreting cells.
Challenges in vaccine development • Choosing the right antigen • Choosing the right adjuvant • Generate the right type of immune response • Elicitation of long-term memory • Financial burden (300-800 million) • Safety • Anti-vaccination • HIV vaccine experience
Overview of the chlamydial developmental cycle, stages at which potential vaccine targets have, or could be, directed, and the immune pathways triggered during chlamydial infection. Panel A describes the seven key stages in the chlamydial developmen... Louise M. Hafner , David P. Wilson , Peter Timms Chlamydia experience http://dx.doi.org/10.1016/j.vaccine.2013.08.020
Chlamydia experience Many chlamydial antigens have been tested, but no single individual one induces sterile protection (Louise M. Hafner , David P. Wilson , Peter Timms, Vaccine 2013) • Polymorphic membrane protein D (pmpD) • Genital tract Th1 cells and IgG2a mucosal antibodies • Eko et al. (2011) [123] • Chlamydial type III-secreted effector protein (Tarp) • Th1 dominant humoral and cellular responses • Wang et al. (2009) [124] • Protein antigens CT823 and CT144 • CD8+ T cell, Th1-polarised CD4 + T cell, Th1-skewed antibody responses • Picard et al. (2012) [125] • MOMP-based serovar E DNA vaccine • Serum IgM, IgG and IgA, CD8+ and CD4+ Tcells in spleen and pelvic lymph nodes • Schautteet et al., 2011 [126] • C. trachomatis serovar D strain pgp3 gene • Humoral (serum IgG) and mucosal IgA anti-Pgp3 antibodies • Comanducci et al. (1994) [127] • Pgp4 gene • Unknown – but the mutant exhibited decreased expression levels of Pgp3, a potential virulence factor amongst others • Song et al. (2013) [55] • TC0052, TC0189, TC0582, TC0660, TC0726, TC0816 and, TC0828 • IgG antibodies with both Th1 and Th2 bias • Molina et al. (2010) [128] • MOMP (CT681), HtrA (CT823), OmcB (CT443), TARP (CT456), GroEL (CT110), Lcr-E (CT089), Nqr3 (TC0551/CT279), MAC-perforin (TC0431/CT153), IncA (TC0396/CT119), and the hypothetical proteins CT622, TC0284, TC0313, TC0651, TC0890, and TC0106 (CT016, CT043, CT372, CT601, and CT733). • Human serum IgG, IFN-γ-producing CD4+ T cells • Finco et al. (2011) [129] • DnaK (CT396) • Human CD4+ T cell responses • Coler et al. (2009) [130] • CT043 • CD4+ Th1 cells • Meoni et al. (2009) [131] • OmcB (CT443) And also CT004, CT043, CT184, CT509, and CT611, CT082, CT089, CT322, CT396, and CT681, CT110 • T cells, B cells or both B and T cells (OmcB) • Follman et al. (2008) [132] • Enolase (CT587) • Human CD4+ T cells • Goodall et al. [133] • Chlamydial protease-like activity factor (CPAF) • CD4 + T cell, IFN-y • Murthy et al. (2006) [134] • NrdB • CD4+ T cells • Barker et al. (2008) [135] • Heat shock protein 60 (cHSP60) • Cervical IgG and IgA antibodies, IFN-g • Agrawal et al. (2007) [136] • Outer Membrane Protein 2 (OMP2) • Humoral antibody responses • Portig et al. (2003) [137]
Antigen versus immune pattern(Chlamydia Experience) • Facts • No single antigen induces full protection • Best results are observed in study using live vaccine candidate in non-human primates • Outcomes are different in infected individuals with different immune response pattern • Question: • Should we focus more on immune response pattern rather than antigen? • What is the best pattern • What is the most efficient way to alter immune response patterns?
Hypothetical, unproven, associations between vaccines and health conditions with country of origin or originator(Andre F, Vaccine 2003)
Frequencies of some scientifically proven serious reactions to vaccines H1N1 vaccine: 6 anaphylaxis cases in Manitoba in 2009
Classification of Potential Vaccines • 1. Live, attenuated vaccines • 2. Vaccines consisting of killed microorganisms • 3. Toxoids • 4. Subunit vaccines • 5. Vectored vaccines (adenoviral, vaccinia virus based, recombinant BCG) • 6. DNA vaccines • 7. Edible vaccines
Table 3 Newer strategies for vaccine development starting from microbial DNA, cDNA or RNA (Plotkin 2005) Strategy Examples of pathogens targeted
Creation of virus like particles (VLP) by recombinant DNA technology • consist of viral protein(s) derived from the structural proteins • These particles resemble the virus from which they were derived but lack viral nucleic acid, thus not infectious • HPV and hepatitis B vaccine • The most recent success in developing papillomavirus vaccine to prevent HPV infection and cervical cancer • Pseudo-particles of human papillomavirus type 16 formed by self-assembly of the L1 viral protein • The VLP elicit high-titers of neutralizing antibodies and other protective immune responses • More immunogenic than soluble proteins
Avian Fluvaccine development by Reverse Genetics techniques • reverse genetics seeks to find the possible phenotypes that may derive from a specific genetic sequence enumerated during DNA sequencing. • engineer change or disruption in DNA sequence and examine the effect of such alterations in the whole organism.
DNA vaccine is particularly efficient in inducing CTL DNA vaccine Protein vaccine
Potential Advantage of DNA Vaccines • - like subunit vaccine (only protective antigen is included but avoid the problem of incorrect folding and glycosylation of antigenic protein • - Stable, less variation and cheaper to prepare. • - Multivalency could be achieved • - Easy inclusion of regulatory cytokines • So far, the results are generally disappointing (better delivery methods and prime/boost approaches are extensively studied now)
Adjuvants and new means of vaccination • Alum • Cytokine/chemokine • CpG • Liposome • Targeting methods (M cell, dendritic cell) • Enlargement of routes of immunization especially for mucosal responses) • Transdermal application (microneedle device)
Mechanism of ISCOM delivery(delivery antigen to cytosol thus activating CD8 T cell through Class I pathway)
Targeting DCs and M cells can enhance protective immune responses
Properties of HIV that hinder vaccine development • Sequence diversity • Infection of critical immune cells • Immune avoidance -Masking of neutralization epitopes -MHC down-regulation -Immune escape through viral mutation - Counter-immunoregulatory mechanisms • Latency
HIV vaccine • All attempts to make a vaccine against HIV-1 have failed. • Three vaccine approaches have been tested in clinical trials for efficacy. • The AIDSVAX glycoprotein (gp)120 vaccine stimulated the production of non-neutralizing antibody to the virus envelope proteins and failed to protect vaccinated individuals from infection. • The STEP vaccine, comprised of three recombinant attenuated adenovirus serotype 5 viruses expressing HIV-1 Gag, Pol and Nef, stimulated CD8+ T cell responses to the viral proteins but again showed no protective effect.
HIV vaccine • A third efficacy trial, in Thailand using a canary pox viral vector expressing gp120, Gag and Pol to prime immune responses followed by the AIDSVAX gp120 vaccine to boost the immune response, has been reported recently. • This showed for the first time a small protective effect, with 30% fewer vaccine recipients becoming infected with HIV-1 than controls. • The volunteer cohort was low risk (annual incidence of infection ~0.3%) and this may be relevant as it may be easier to protect such people than those at high risk. • It is not clear whether protection was mediated by antibody, T cells, innate cells or some combination of the three, but those who did become infected did not have reduced virus levels, which is usually seen for protection mediated by T cells in SIV models.
HIV vaccine • RV 144, or the Thai trial, is the name of an HIV vaccine clinical trial combining two vaccines that failed on their own (gp120) • 16,402 Thai volunteers aged 18–30 • This trial give the first supporting evidence of any vaccine being effective in lowering the risk of contracting HIV (31% protection) • Activation of immune cells?
Critical points in future HIV vaccine development • Future vaccine approaches should be less empirical and a deeper understanding of the earliest immune responses to HIV-1 and SIV infection is needed. • It will be important to understand why broad-specificity, neutralizing antibodies are not routinely induced and to determine ways to safely induce them, and to identify what immune responses lead to a better outcome • It is also important to know why the rare individuals, known as 'elite controllers', can successfully control HIV-1 infection for decades without needing antiretroviral drug therapy
Further Readings • Janeway, Immunobiology, 6th ed, p642-657. • Stanley Plotkin, Vaccines: past, present and future. Nature Medicine 11:S5-11, 2005 • Sarah Gilbert: T cell-inducing vaccines-What’s the future? Immunology 135:19-26, 2012