Download
1 / 16
200 likes | 593 Vues
Lateral Ankle Pathology. Brent Ricks DPM . Overview. Anatomy Clinical presentation Ankle Sprain classification Conservative treatment Surgical treatment Conclusion. http://www.sliceofscifi.com/2008/03/25/oh-yeah-they-know-were-here/. Anatomy 8,11. Anterior Talofibular Ligament

E N D
Lateral Ankle Pathology Brent Ricks DPM
Overview • Anatomy • Clinical presentation • Ankle Sprain classification • Conservative treatment • Surgical treatment • Conclusion http://www.sliceofscifi.com/2008/03/25/oh-yeah-they-know-were-here/
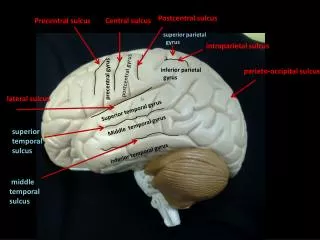
Anatomy8,11 • Anterior Talofibular Ligament • Intracapsular 10mm proximal from the Fibular tip • Controls anterior movement of Talus • Most important stabilizer for inversion • Anatomically weakest of the three lateral ankle ligaments Involved three times more than the CFL • Calcaneofibular ligament • Most important stabilizer of STJ • Extracapsular deep to Peroneals • Posterior Talofibular ligament • Intracapsular • Rarely injured • Peroneal tendons http://www.bodyassist.com/content.php?page=tapeanankle
Clinical Presentation8,10,11,12,15 • Subjective • 85% acute ankle sprains are plantarflexion inversion • 10-40% of Acute ankle sprains will continue to chronic ankle instability • Pain, weakness, crepitus, instability, swelling, stiffness • Objective • Rearfoot varus, plantar flexed first ray, Cavus foot • Peroneal tear and or strength deficit • STJ instability in 10-75% • Tibiofibular syndesmosis • Injured 1-18% in ankle sprains, most commonly seen in collision sports • Pain in anteriolateral ankle with increased pain with dorsiflexion • Frick test; Hold foot in neutral and externally rotate the foot on a fixed leg. Pain over the syndesmosis (recreates the mechanism of injury) • Squeeze Tibia and Fibula together at midpoint of calf. Pain is at distal Tib-Fib syndesmosis • Anterior Drawer • Suction or Sulcus sign over ATFL • 10mm bil or 3mm difference • Talar Tilt (CFL) • 9 degree absolute, 3 difference • Talar dome lesions/Ankle arthritis • (20/30, 8/28) http://www.tabers.com/tabersonline/ub/view/Tabers/143062/29/ANTERIOR_DRAWER_TEST http://ajs.sagepub.com/content/36/6/1143.abstract
Ankle Sprain Classification2 • Grade 1- Little swelling and tenderness, minimal or no functional loss, no mechanical joint instability • Grade 2- Moderate pain, swelling over the involved structures, loss of some joint motion with mild to moderate joint instability • Grade 3- complete ligament rupture with marked swelling, hemorrhage and tenderness, loss of function, joint motion and instability http://www.ankleandfootnorthwest.com/ankle-sprain.html http://www.atlantisfootandankle.com/ankle-sprain-instability.aspx
Conservative treatment2,3,4,5,9 • RICE until swelling and pain resolves then ankle mobilization and early weight bearing • Cryotherapy with in 36 hours returned to full activity in 13.2 days vs. 30.4 days beginning after 36 hours • NSAIDS • Taping effectiveness decreases 40% after 10min of exercise, no significant support after 60 min. • Taping helps minimize motion, if previously injured more than to an uninjured ankle, within 30 min window • Ankle braces demonstrate no significance with those who had a previous injury in high school volleyball. • A rigid brace in previously uninjured females may help http://www.ehow.com/video_9595_tape-sprained-ankle.html http://www.countrforce.com/sportanklebrace.html
Conservative Treatment1,2 • PT • Grade 1-2- A functional program should start immediately (3 weeks after injury to maximize collagen content) • Unilateral stance on a soft surface for kinesthetic awareness • Agility ladder for timing coordination • Tilt board for proprioceptive and Peroneal strengthening to improve functional instability (giving out) • Plyometric exercises (eccentric loading immediately followed by concentric contraction) are more effective in increasing functional performance than strength training • Complex series of hops and jumps • Strength training • Inversion, eversion, dorsiflexion, plantarflexion against resistance; Heel rise/ toe rise; towel curl, marble pick up • Activities without PT monitoring resulted in less effectiveness and were performed correctly 50% of the time http://www.uksoccershop.com/p-17410/power-speed-parachute.html http://www.extraedgetraining.com/blog/2010/04/under-rated-training-equipment/ http://www.sgwoodworksllc.com/Products-2.html
Conservative Treatment6,7 • Orthotics • Pt with chronic ankle instability have lateral foot biased weight distribution in walking and barefoot running • Any medial ground reactive force should be avoided. • High arched Pt that flattens with weight bearing should get maximum arch fill on cast • Oblique valgus post • Reduce PTF and CFL tension • 3 degrees for Pt with Calcaneous aligned under leg, more for pes cavus • Valgus forefoot post • Cuboid pad to decrease ATFL tension • Lateral clip http://www.wecreatewellness.com/orthotics/ http://www.sportsinjuryclinic.net/cybertherapist/general/pronate.htm
Surgical Treatment8,11 • Brostrom-Gould • Midsubstance repair • Incorporation of inferior extensor retinaculum • Mild to moderate instability • 85-95% effective in treating chronic instability • Superior to tenodesis for functional outcomes http://www.google.com/imgres?q=brostrom+ligament+repair&um=1&hl=en&qscrl=1&nord=1&rlz=1T4DKUS_enUS274US275&biw=1427&bih=827&tbm=isch&tbnid=8yoHzXkjf8HzBM:&imgrefurl=http://www.medscape.com/viewarticle/535715_2&docid=xDV28YmYCTczaM&w=550&h=577&ei=DudGTqb2B-KIsgKWyoSSCA&zoom=1&iact=rc&dur=78&page=1&tbnh=156&tbnw=149&start=0&ndsp=24&ved=1t:429,r:0,s:0&tx=90&ty=67
Kang SK et al. Long-Term Results After Modified Brostrom Procedure Without Calcaneofibular Ligament Reconstruction. Foot and Ankle International. 2011 (32) 153-157 • 26/30 male patients • Average age 23 • 80% high level or amateur athletes • 6 months conservative treatment with more than 15mm anterior drawer • ATFL repair at anterior fibular border with extensor retinaculum anchor to periosteum. • Short leg cast 4 weeks • Air Cast ankle brace 2 weeks • At 4 weeks gentle ROM • PT at 6 weeks • Full weightbearing when full ankle ROM reached http://www.myfootshop.com/detail.asp?condition=ankle%20sprain
Kang SK et al. Long-Term Results After Modified Brostrom Procedure Without Calcaneofibular Ligament Reconstruction. Foot and Ankle International. 2011 (32) 153-157 • Follow up 10.6 years • Excellent (asymptomatic, full activities) • 12/30 patients • Good (some symptoms, full activity) • 16/30 patients • Fair (symptomatic not fully functioning) • 2/30 patients (re-injured) • No statistical difference in ROM in contralateral ankle • Anterior Drawer • Grade 0 (<5mm) - 13 • Grade 1 (5-10mm) - 13 • Grade 2 (10-15mm) - 4 http://blog.syracuse.com/sports/2011/07/us_womens_soccer_team_has_hist.html
Surgical Treatment8,11 • Chrisman-Snook • Split Peroneous Brevis does not result in loss of eversion strength • 80% good to excellent results • Indications • Failed Brostrom, significant instability, Morbidly obese, STJ instability • Non-weight bearing 4 weeks followed by protected weight bearing as tolerated • Non-weight bearing 1 week. CAM boot with advancement of weight bearing until 6th week. Light exercise until 3months out. • Free Semitendinosus allograft anchored to the lateral Talar neck • Gracilis tendon autograft Watson Jones Evans http://www.lexikon-orthopaedie.com/pdx.pl?dv=0&id=01620
Klammer et al. Percutaneous Lateral Ankle Stabilization: An Anatomical Investigation. Foot and Ankle International. 2011 (32) • Cadavaric study, 11 feet, Gracilis graft • 5mm incision at the anterior margin of the Fibula 10-15mm proximal of the Fibular tip • Guide wire into the Talar neck used to guide the bone tunnel • Tendon graft inserted and secures with absorbable interference screw • Fibular tunnel then created at the same level • Second incision made at the posterior Fibular tunnel and graft passed • 3rd incision at the insertion of CFL, Posterior and superior to Peroneal tubrical, and tunnel through Calcaneous made • Tendon passed and secured • Medial Calcaneal Branch of the Tibial nerve hit 2/11. No other nerovascular structures were compromised http://www.auntminnieeurope.com/index.aspx?sec=sup&sub=mri&pag=dis&itemId=605243
Surgical Treatment9 • Peroneal Repair • Brevis more commonly involved • Less than 50% of tendon torn • primary repair, debridement, tubularization • More than 50% torn • Tendon grafting • Side to side anastomosis • Tendonosis • Debridement • Topaz, PRP, etc http://radiographics.rsna.org/content/20/suppl_1/S153.full http://www.footankleinstitute.com/peroneal-tendon-tear/
Conclusion • RICE with immobilization and NSAID, PT • Orthosis and braces • Consider all structures of lateral ankle, best viewed with MRI • Brostrom Gould for ATF and CFL repair and augmentation • If that fails, STJ instability, obesity; Tenodesis
References • Hawson ST. Physical Therapy and Rehabilitation of the Foot and Ankle in the Athlete. Clin Podiatr Med Surg. 2011; 189-201 • Ismail MM; Ibrahim MM; Youssef EF; El Shorbagy KM. Plyometric Training Versus Resistive Exercises After Acute Lateral Ankle Sprain. Foot and Ankle International. 2010; (31) 523-530 • Frey C; Feder KS; Sleight J. Prophylactic Ankle Brace use in High School Volleyball Palyers: A Prospective Study. Foot and Ankle International. 2010; (31) 296-300 • Hubbard TJ; Cordova M. Effect of Ankle Taping on Mechanical Laxity in Chronic Ankle Instability. Foot and Ankle International 2010; (31) 499-504 • Lyrtzis C; Natsis K; Papadopoulos C; Noussios G; Papathanasiou E. Efficacy of Paracetamol Versus Diclofenac for Grade 2 Ankle sprins. Foot and Ankle International. 2011; (32) 501-575 • Morrison KE; Hudson DJ; Davis IS; Richards JG; Royer TD; Dierks TA; Kaminski TW. Plantar Pressure During Runnig in Subjects with Chronic Ankle Instability. Foot and Ankle International. 2010 (31) 994-1000 • Rosenbloom KB. Pathology-Designed Custum Molded Foot Orthoses. Clin Podiatr Med Surg. 2011 (28) 171-187 • Hentges MJ; Lee MS. Chronic Ankle and Subtalar Loint Instability in the Athlete. Clin Podiatr Med Surg. 2011 (28) 87-104 • Franson J; Baravarian B. Lateral Ankle Triad: The triple Injury of Ankle Synovitis, Lateral Ankle Instability, and Peroneal Tendon Tear. Clin Podiatr Med Surg. 2011 (28) 105-115 • Soomekh DJ. New Technology and Techniques in the Treatment of Foot and Ankle Injuries. Clin Podiatr Med Surg. 2011 (28) 19-41 • Schenck RC; Coughlin MJ. Lateral Ankle Instability and Revision Surgery Alternatives in the Athlete. Foot Ankle Clin N AM. 2009 (14) 205-214 • Lee KT; Park YU; Kim JS; Kim JB; Kim KC; Kang SK. Long-Term Results After Modified Brostrom Procdure Without Calcaneofibular Ligamnet Reconstruction. Foot and Ankle International. 2011 (32) 153-157 • Klammer G; Schlewitz G; Stauffer C, Vich M; Espinosa N. Percutaneous Lateral Ankle Stabilization: An Anattomical Investigation. Foot and Ankle International. 2011 (32) 66-70 • Irwin TA; Anderson RB; Davis WH; Cohen BE. Effect of Ankle Arthritis on the Clinical Outcome of Lateral Ankle Ligament Reconstruction in Cavovarus Feet. Foot and Ankle International. 2010. (31) 941-948