Download
1 / 20
200 likes | 430 Vues
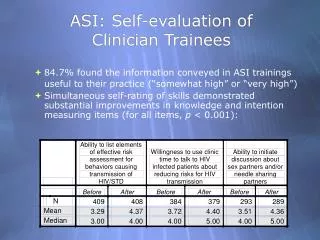
Comparing Clinician Evaluation of mild TBI history with ACRM Criteria. Terri Krangel Pogoda, PhD 1 Ann Hendricks, PhD 1 Errol Baker, PhD 1 John A. Gardner, PhD 1 Katherine M. Iverson, PhD 1 Maxine H. Krengel, PhD 1 Mark Meterko, PhD 1 Kelly L. Stolzmann, MS 1 Henry L. Lew, MD, PhD 2.

E N D
Comparing Clinician Evaluation of mild TBI history with ACRM Criteria Terri Krangel Pogoda, PhD1 Ann Hendricks, PhD1 Errol Baker, PhD1 John A. Gardner, PhD1 Katherine M. Iverson, PhD 1 Maxine H. Krengel, PhD1 Mark Meterko, PhD1 Kelly L. Stolzmann, MS1 Henry L. Lew, MD, PhD2 1VA Boston Healthcare System2Defense and Veterans Brain Injury Center This work is supported by VA HSR&D Grant: SDR 08-405
Disclaimer The views expressed in this presentation are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
OEF/OIF Veterans and Traumatic Brain Injury (TBI) • High risk of TBI during OEF/OIF deployments • Blow to the head that disrupts brain functioning • Prevalence: 12-20%1-4 • Most cases are mild in severity5 • Postconcussive symptoms6 • In OEF/OIF Veterans…7 • Posttraumatic Stress Disorder (PTSD) (58.2%) • Anxiety (28.3%) • Depression (42.3%)
ACRMCriteria for identifying TBI8,9 A traumatically induced physiological disruption of brain function, as manifested by at least one of the following: • Loss of consciousness (LOC) • Alteration of consciousness (AOC) • Posttraumatic amnesia (PTA) • Focal neurologic deficit(s) that may or may not be transient (e.g., weakness, loss of balance, change in vision) • Intracranial lesion
Study Aims 1) To identify concordance rates of VA clinician judgment of deployment-related mTBI history with ACRM criteria 2) To identify variables associated with clinician errors (misses, false positives) in evaluating mTBI history
Data Source: Comprehensive TBI Evaluation (CTE) • Protocol to assist in making a clinical judgment about whether a TBI occurred (mostly self-report) • Etiology of injury • Blast • Non-blast (i.e. vehicular accidents, bullet wound, falls, other blunt trauma) • Post-injury sequelae (LOC, AOC, PTA) and their duration • Presence of probable psychiatric comorbidity • 22-item Neurobehavioral Symptom Inventory(NSI-22)10
Study sample • Veterans who… • Completed a CTE between FY 2008 and FY 2009 • Been judged to have or not have deployment-related mTBI • Did not report TBI prior to or following deployment • Sample of 19,669 Veterans for analysis who had data from both ACRM criteria and clinician judgment of mTBI history
Design • Retrospective database review • Outcome variables • Concordance rates of clinician judgment of mTBI history with ACRM criteria • Misses vs. True Positives • False Positives vs. True Negatives • Independent Variables • Demographics • Deployment-related events • Mental health judgments • NSI-22 symptoms • Descriptive statistics and logistic regressions
Results Table 1. Sample Characteristics (N = 19,669) *Based on CTE data
Figure 1. Nsi-22 subscale scores by outcome Severe * * * * None *True Positive > (False Negative = False Positive) > True Negative
Table 3: Logistic regressions ‡p < .10, *p < .05, **p < .01, ***p < .001, ****p < .0001
Summary • The majority of mTBI history evaluations reviewed agreed with ACRM criteria: 71.9% either true positives or true negatives. • Clinician judgment of mTBI history sensitive to deployment-related injuries, mental health conditions, and cognitive and somatosensory symptoms. • For misses, it is possible that clinicians may be misinterpreting NSI-22 affective complaints (e.g., fatigue, irritability, sadness) as being related to readjustment issues, rather than mTBI history.
Limitations • Nature of clinician-patient conversations that led to clinical decision unknown. • Do not know the basis of evaluator’s judgment about mental health conditions. • Data are from FY2008-09, may not reflect current evaluation practices.
Implications, considerations, future directions • Automating CTE template to populate TBIhistory question based on AOC, LOC, PTA • More consistent rates of: • TBI history (Q23) • TBI symptom persistence (Q23a) • TBI symptom resolution (Q23a) • How do misses (26.1%) and false positives (2.0%)impact referrals, utilization, and outcomes? • Variability in the implementation of the CTE process
Contact Information • My contact information: terri.pogoda@va.gov • HSR&D PI’s contact information: ann.hendricks@va.gov
References • Hendricks, A., Amara, J., Baker, E., Charns, M., Gardner, J. A., Iverson, K. M., Kimerling, R., Krengel, M., Meterko, M., Pogoda, T. K., Stolzmann, K. L., Wolfsfeld, L., & Lew, H. L. (2010). Screening for mild Traumatic brain injury in OEF-OIF deployed military: An empirical assessment of the VA Experience. Unpublished manuscript. • Hoge, C. W., McGurk, D., Thomas, J. L., Cox, A. L., Engel, C. C., & Castro, C. A. (2008). Mild traumatic brain injury in U.S. soldiers returning from Iraq. New England Journal of Medicine, 358, 453-463. • Schneiderman, A. I., Braver, E. R., & Kang, H. K. (2008). Understanding sequelae of injury mechanisms and mild traumatic brain injury incurred during the conflicts of Iraq and Afghanistan: Persistent postconcussive symptoms and posttraumatic stress disorder. American Journal of Epidemiology, 167, 1446-1452. • Tanielian, T., & Jaycox, L. H. (2008). Invisible wounds of war: Psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corp. • Hoge, C. W., Goldberg, H. M., & Castro, C. A. (2009). Care of war Veterans with mild traumatic brain injury—Flawed Perspectives. New England Journal of Medicine, 360, 1588-1591. • Sayer, N. A., Rettmann, N. A., Carlson, K. F., Bernardy, N., Sigford, B. J., Hamblen, J. L., Friedman, M. J. (2009). Veterans with history of mild traumatic brain injury and posttraumatic stress disorder: Challenges from provider perspective. Journal of Rehabilitation Research & Development, 46, 703-716. • Carlson, K. F., Nelson, D., Orazem, R. J., Nugent, S., Cifu, D. X., & Sayer, N. A. (2010). Psychiatric diagnoses among Iraq and Afghanistan war veterans screened for deployment-related traumatic brain injury. Journal of Traumatic Stress, 23, 17-24. • Kay T, Harrington DE, Adams R. Mild Traumatic Brain Injury Committee, American Congress of Rehabilitation Medicine, Head Injury Interdisciplinary Special Interest Group’s definition of mild traumatic brain injury. J Head Trauma Rehabil. September 1993;8:86-87. • Department of Veterans Affairs and Department of Defense. VA/DoD Clinical Practice Guideline for Management of Concussion/Mild Traumatic Brain Injury Washington, DC April 2009. • Cicerone, K. D., & Kalmar, K. (1995). Persistent postconcussion syndrome: The structure of subjective complaints after mild traumatic brain injury. Journal of Head Trauma Rehabilitation, 10, 1–17. • Meterko, M., Baker, E., Stolzmann, K. L., Cicerone, K. D., Hendricks, K. M., & Lew, H. L. (2010). Psychometric assessment of the NSI-22. Unpublished manuscript.